If you are reading this before your first infusion, I want you to know two things. First: you are asking exactly the right question, at exactly the right time, and far too few people do. Second: there are real, evidence-backed things you can do to lower your risk of nerve damage from chemotherapy — and there is also a lot of hopeful-sounding noise you can safely ignore.
I'm Janet Ellis. I write here as a community advocate who has lived with neuropathy for years, not as a doctor or oncologist. What follows is what the research actually shows about protecting your nerves during cancer treatment, sorted honestly into “worth asking your team about,” “promising,” and “skip it.” Bring this to your oncology team. The decisions belong with them — but you can walk in already knowing the right questions.
First, the Honest Truth About “Prevention”
Chemotherapy-induced peripheral neuropathy, often shortened to CIPN, is one of the most common and most under-discussed side effects of cancer treatment. Depending on the drugs used, somewhere around a third or more of people treated with the nerve-toxic agents develop some degree of it — numbness, tingling, burning, or a “gloves and socks” loss of sensation in the hands and feet.
No pill reliably prevents chemo neuropathy. The levers that actually work are not supplements — they are early symptom reporting, dose decisions made with your oncologist, and simple physical strategies during infusion. The realistic goal is lower risk and milder symptoms, not a guarantee.
Here is the part the internet often gets wrong: as of today, no medication or supplement is recommended by major oncology guidelines as a reliable way to prevent CIPN. The leading professional guideline reviewed the evidence and could not endorse a single preventive drug. So if you read that a particular pill “prevents chemo neuropathy,” be skeptical.
That does not mean you are powerless. It means the things that genuinely move the needle are not pills — they are timing, dose decisions made with your oncologist, and a few simple physical strategies during infusion. Lowering risk and lessening severity are realistic goals. A guarantee is not. Holding both of those truths at once is the right mindset walking in.
Which Chemotherapy Drugs Damage Nerves
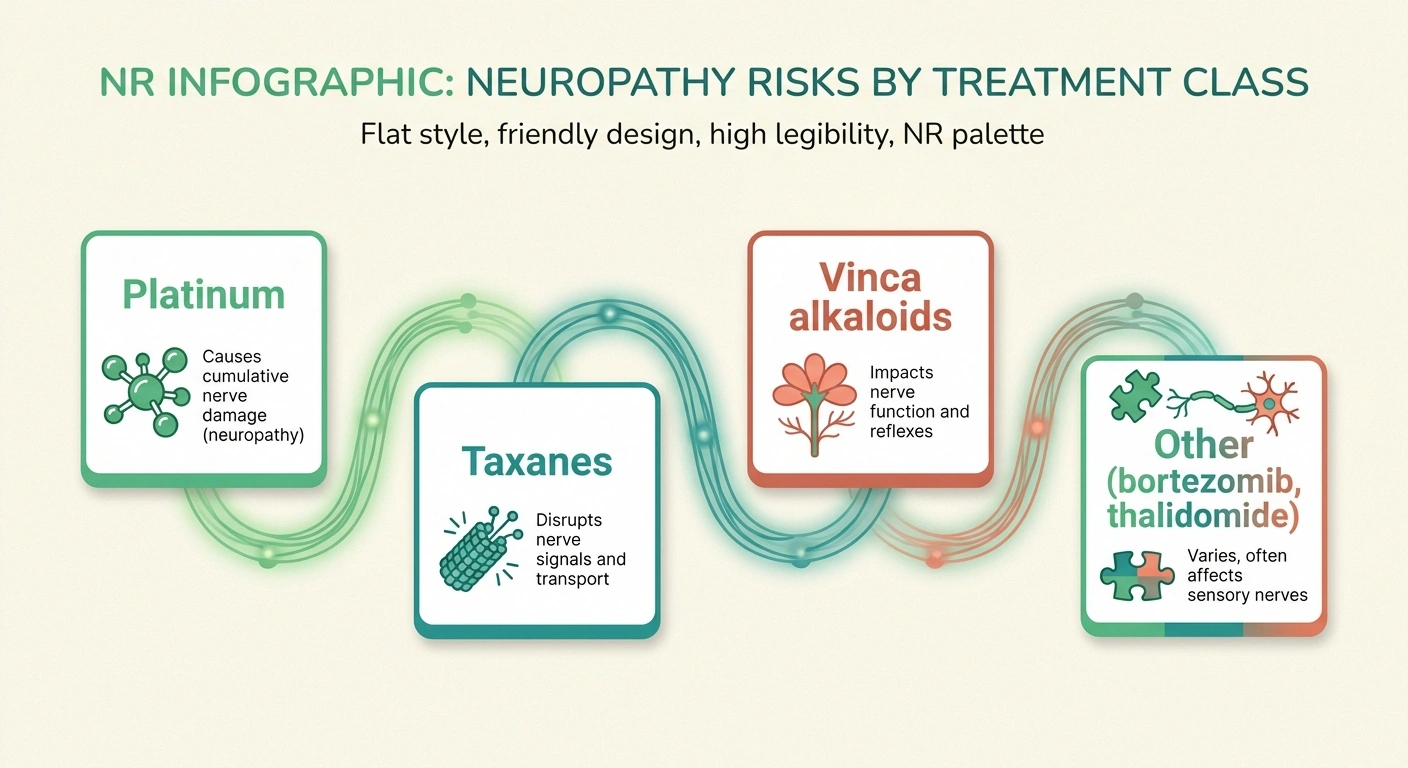
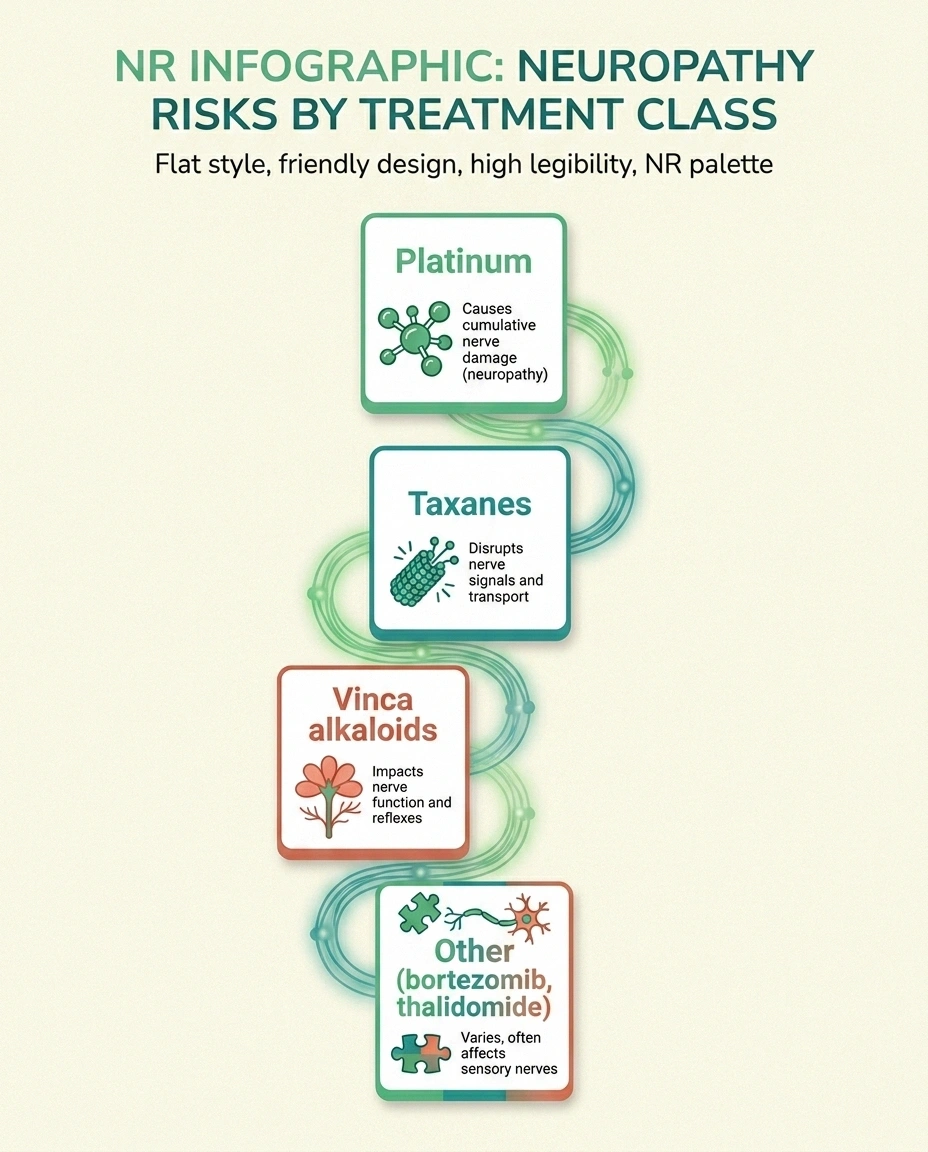
Not every chemotherapy regimen carries the same risk. The agents most associated with nerve damage fall into a few families:
Chemotherapy Drug Families That Commonly Affect Nerves
Ask your oncologist: “Does my regimen include a drug that commonly causes neuropathy, and which one?”
- Platinum drugs — oxaliplatin, cisplatin, carboplatin. Oxaliplatin is notable for an acute, cold-triggered nerve reaction during and shortly after infusion, on top of a longer-term form.
- Taxanes — paclitaxel, docetaxel, nab-paclitaxel. A very common cause, especially in breast and ovarian cancer regimens.
- Vinca alkaloids — vincristine, vinblastine.
- Proteasome inhibitors — bortezomib, used in multiple myeloma.
- Thalidomide and related drugs.
Why does this list matter to you? Because the first useful question you can ask your oncologist is simply: “Does my regimen include a drug that commonly causes neuropathy, and if so, which one?” Knowing the answer tells you how closely to watch, and which of the strategies below are even relevant. If you want a deeper look at how this kind of nerve damage develops and feels, our guide to chemotherapy-induced neuropathy (CIPN) walks through it in detail.
The Single Most Powerful Protection: Speaking Up Early
If you take only one thing from this article, take this. The most effective protective lever in all of CIPN is not a supplement or a cooling glove. It is early reporting and the dose adjustment that follows it.
Report numbness, tingling, buzzing, or clumsiness the week it starts — not the month it becomes unbearable. Caught early, your oncologist can adjust the dose, schedule, or drug. Reporting early does not mean undertreatment; it means the trade-offs get made deliberately, by the right person, with your input.
Nerve damage from chemotherapy tends to accumulate. Caught early, while it is mild tingling, an oncologist can sometimes reduce the dose, change the infusion schedule, switch agents, or pause — decisions that can stop mild symptoms from becoming permanent ones. The tragedy of CIPN is how often patients minimize early symptoms, push through because they do not want to jeopardize their cancer treatment, and only report it once it is severe and harder to reverse.
So: tell your team about numbness, tingling, buzzing, or clumsiness the week it starts, not the month it becomes unbearable. You are not being difficult. You are giving your oncologist the one window where the most powerful intervention — a treatment adjustment that only they can make — actually works. Reporting early does not mean your cancer will be undertreated; it means the trade-offs get made deliberately, by the right person, with your input.
Cryotherapy — Cooling Hands and Feet During Infusion

Cryotherapy means wearing frozen gloves and socks (or cooling devices) on your hands and feet during certain infusions. The idea is that cooling narrows blood vessels in the extremities, so less of the nerve-toxic drug reaches the small nerves in your fingers and toes during the window it is circulating at high levels.
This is one of the more encouraging areas of research. Meta-analyses looking at taxane chemotherapy have found that cryotherapy can reduce the incidence of peripheral neuropathy, and recent clinical guidance lists it among the more promising practical options. It is low-risk for most people, though it is genuinely uncomfortable and not appropriate for everyone — people with cold-sensitivity conditions, for example, or those on oxaliplatin, where cold itself triggers symptoms.
This is exactly the kind of thing to raise with your infusion team, because availability varies by center and the suitability depends on your specific drug. You can read more about how cold is used therapeutically — and its limits — in our overview of cryotherapy for neuropathy.
Compression Therapy — A Simple, Promising Option

Compression therapy — wearing snug surgical gloves or compression sleeves on the hands and feet during infusion — works on a similar principle to cryotherapy: gently limiting blood flow to the extremities during the high-concentration window. It has the advantage of being far more comfortable than ice.
A systematic review and meta-analysis pooling several randomized trials found that compression therapy reduced the incidence of CIPN, and notably also reduced depression, with high patient adherence — unsurprising, since it is much easier to tolerate than frozen gloves for hours. The evidence is rated as moderate, which in this field is meaningfully strong. Because it is simple, cheap, and well-tolerated, it is a reasonable thing to ask whether your center offers, particularly for taxane regimens.
Exercise During Treatment — The Best-Supported Habit

Of all the things you can personally do, structured exercise during treatment has some of the most consistent research behind it. Systematic reviews of aerobic and resistance exercise during chemotherapy have found modest but real reductions in CIPN symptom severity, along with better balance, function, and quality of life — and balance matters enormously, because numb feet plus poor balance is a fall risk.
Where the Evidence Stands
“Exercise” here does not mean training for a marathon during chemo. It means a supervised or guided program of gentle aerobic movement and light resistance work, scaled to how you feel on a given day and cleared by your care team. Many cancer centers have exercise oncology or physical therapy programs designed precisely for people in active treatment — ask for a referral. To see what nerve-protective movement looks like in practice, our complete guide to the best exercises for neuropathy is a good starting frame, and our piece on balance and fall prevention covers the safety side.
What About Supplements and Vitamins?

This is where I have to be most direct, because this is where the most money is spent on the least evidence. Vitamin E, glutathione, calcium and magnesium infusions, alpha-lipoic acid, and acetyl-L-carnitine have all been studied for preventing CIPN. The honest summary: none is recommended for prevention by the leading guideline, and the evidence for most is inconsistent or negative.
Acetyl-L-carnitine, often marketed for “nerve health,” was studied for CIPN prevention and may actually worsen neuropathy in the chemo setting. “Natural” and “for nerves” on a label does not mean safe during chemotherapy. Review every supplement with your oncology team before continuing it.
One deserves a specific safety warning. Acetyl-L-carnitine, sometimes marketed for nerve health, was studied for CIPN prevention and the trial suggested it may actually worsen neuropathy in this setting. That is a striking example of why “natural” and “for nerves” on a label does not mean “safe to add during chemo.” Anything you take during treatment — including supplements you have taken for years — should be reviewed with your oncology team, because some can interfere with chemotherapy itself.
This is not the same as saying supplements never have a role in neuropathy generally; for non-chemo nerve health some have a reasonable evidence base, which we cover in our guide to the best neuropathy supplements for nerve health and specifically alpha-lipoic acid. But “helpful for general nerve health” and “prevents chemo neuropathy” are different claims, and the chemo setting is the one where unsupervised supplementing can backfire. A nutrient-focused, anti-inflammatory eating pattern is a gentler, safer lever — see diet for neuropathy prevention.
After Treatment: What Recovery Actually Looks Like
For many people, CIPN improves in the months after chemotherapy ends, as nerves slowly recover. For some, it improves only partially, or persists. Recovery is usually slow and uneven, measured in months and seasons rather than weeks, and it is one of the reasons early reporting during treatment matters so much — the symptoms you prevent from becoming severe are the ones least likely to become permanent.
If symptoms linger after treatment, the focus shifts from prevention to management, and that is a different and more hopeful conversation: pain control, physical therapy, balance work, footwear, and the day-to-day strategies that make life with residual numbness manageable. The point of everything above is to walk out of treatment with as little of that to manage as possible.
Questions to Bring to Your Oncology Team
You do not need to memorize the science. You need a short list of questions that turns all of this into a real conversation:
Bring This List to Your Next Appointment
- Does my chemotherapy regimen include a drug that commonly causes neuropathy? Which one?
- How will we monitor my nerves, and exactly what symptoms should make me call you — and how soon?
- Does this center offer cryotherapy or compression during infusion, and am I a candidate given my specific drug?
- Can you refer me to an exercise oncology or physical therapy program for during treatment?
- Here is everything I currently take, including supplements — is anything a problem to continue during chemo?
- If I do develop symptoms, what are my options for adjusting treatment, and how do we weigh that against cancer control?
Walking in with that list changes the dynamic. You are no longer a passenger hoping nothing goes wrong; you are a participant in the decisions that protect you. That shift, more than any single intervention, is what good outcomes tend to have in common.
Frequently Asked Questions
Can chemotherapy-induced neuropathy be completely prevented?
No intervention reliably prevents it, and no major oncology guideline endorses a preventive medication. The realistic goal is to lower your risk and reduce severity through early symptom reporting, treatment adjustments made by your oncologist, and physical strategies like cryotherapy, compression, and exercise. Lowering risk is achievable; a guarantee is not.
What is the single most effective thing I can do?
Report early symptoms immediately. Nerve damage from chemotherapy accumulates, and catching it while it is still mild gives your oncologist the window to adjust the dose, schedule, or drug — the most powerful protective lever there is. Pushing through and reporting it late is the most common avoidable mistake.
Do frozen gloves and socks really work?
For taxane chemotherapy, meta-analyses suggest cryotherapy can reduce the incidence of neuropathy, and recent guidance lists it as promising. It is low-risk for most people but uncomfortable, and it is not appropriate for everyone — particularly people on oxaliplatin, where cold itself triggers symptoms. Whether it suits your specific regimen is a question for your infusion team.
Should I take alpha-lipoic acid or acetyl-L-carnitine during chemo to protect my nerves?
Not without your oncology team's approval. Neither is recommended for preventing CIPN, and acetyl-L-carnitine was found in a study to possibly worsen neuropathy in the chemo setting. Some supplements can also interfere with chemotherapy itself. Review everything you take with your team before continuing it during treatment.
Is exercise safe during chemotherapy?
For most people, gentle structured exercise during treatment is not only safe but beneficial, with research showing reduced CIPN severity and better balance and quality of life. It should be scaled to how you feel and cleared by your care team; many cancer centers have exercise oncology or physical therapy programs designed for this.
Will the neuropathy go away after chemotherapy ends?
For many people it improves over the months following treatment as nerves slowly recover, though for some it improves only partially or persists. Recovery is typically slow and uneven. Symptoms kept mild during treatment through early reporting are the ones most likely to resolve.
If I report symptoms, will my cancer be undertreated?
Reporting symptoms early does not mean treatment is automatically reduced. It means the trade-off between cancer control and nerve protection gets made deliberately, by your oncologist, with your input — rather than by accident because no one knew the damage was happening. That is a better position, not a worse one.