If you've sat in a neurologist's office and heard the words “length-dependent neuropathy,” you may have nodded politely and walked out still wondering what they actually meant. I did, the first time. It sounded like a technical label that somehow explained nothing.
But once I understood it, the shape of my whole illness made sense. Why my toes went first. Why my hands came later. Why the numbness climbs up the legs like a tide, not a wave. And most importantly — what this pattern tells us about the kind of nerve damage you probably have, and what that means for treatment and watching for red flags.
Let me walk you through it the way I wish someone had walked me through it.
What “Length-Dependent” Actually Means
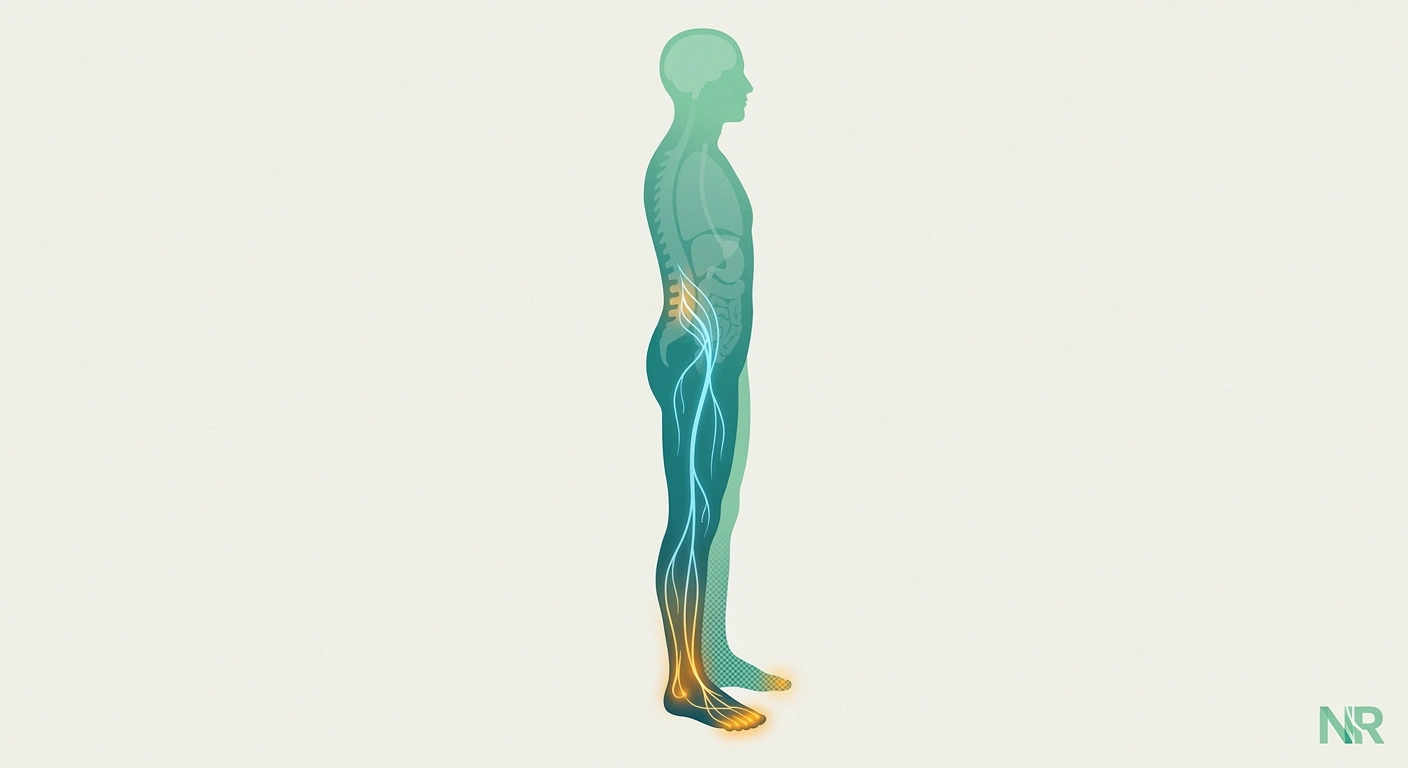
The word sounds intimidating but the idea is almost elegantly simple. Your longest nerves are damaged before your shorter ones. In medical language, this is sometimes called a “dying-back” pattern or a “distal axonopathy.” The axon — the long wire-like extension of the nerve cell — begins to break down at its farthest tip and the damage slowly works its way back toward the cell body.
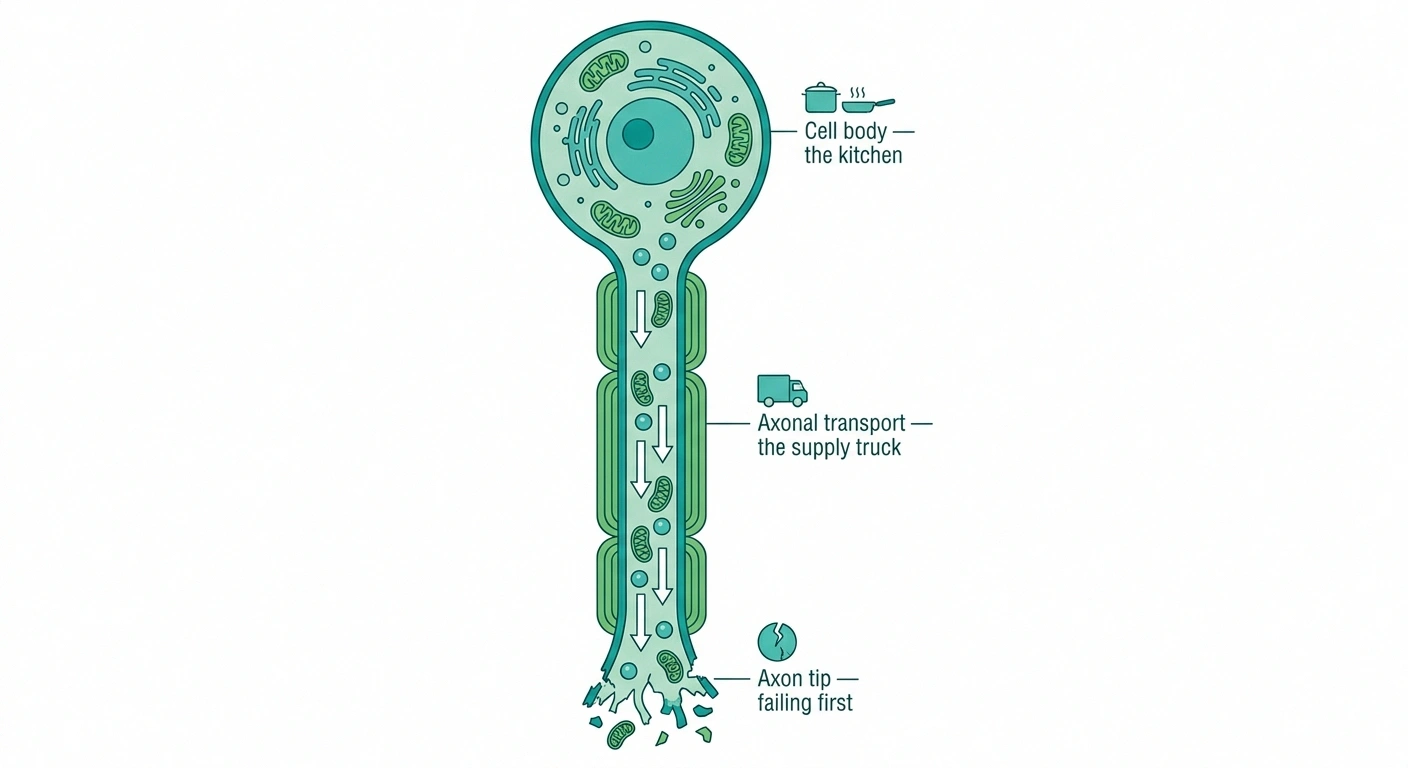
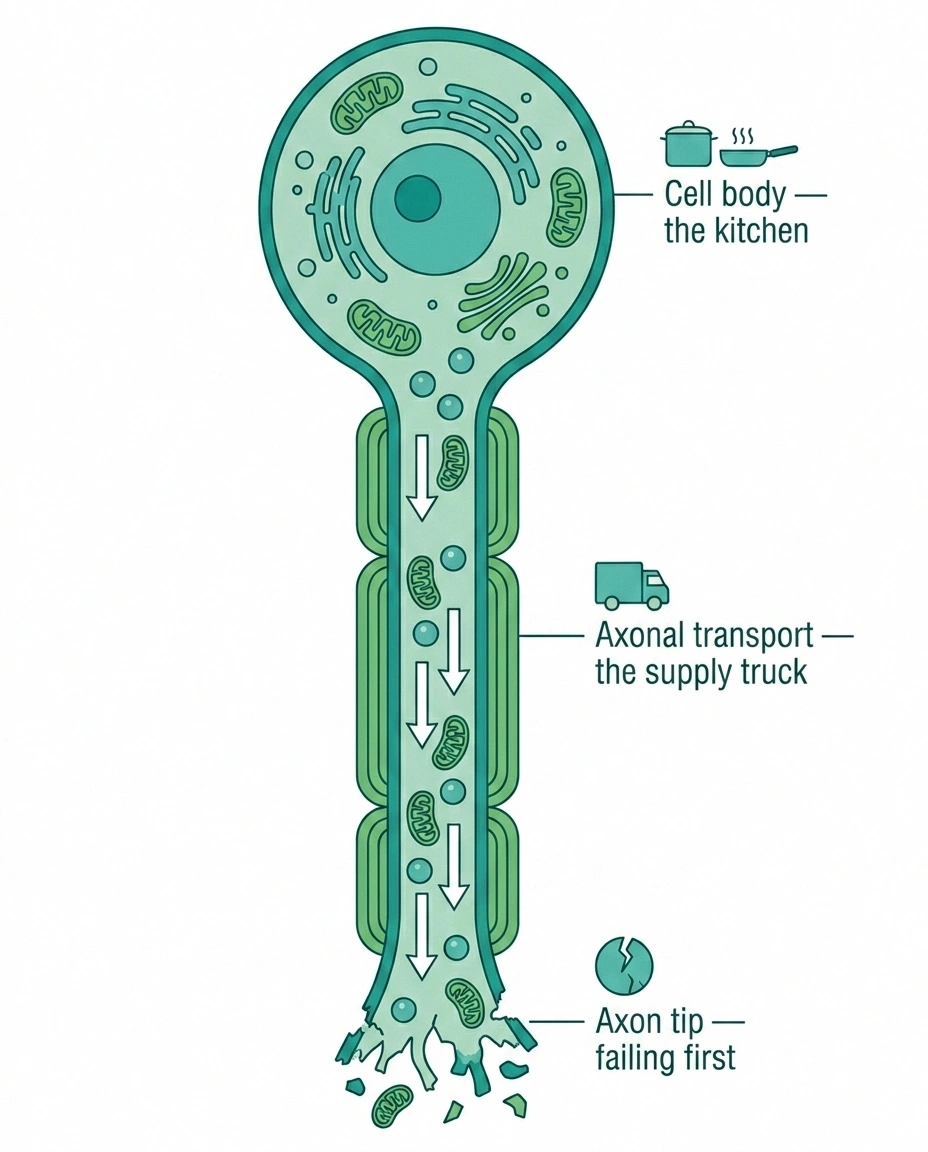
Your longest peripheral nerves run from the lower spine all the way to your toes. For a person of average height, that's close to one meter of axon that has to be fed, repaired, and maintained from a single cell body sitting up in the lumbar region. When something goes wrong with the body's ability to support that cell — toxins, high blood sugar, a vitamin deficiency, chemotherapy — the first parts to suffer are the parts farthest from the “kitchen.”
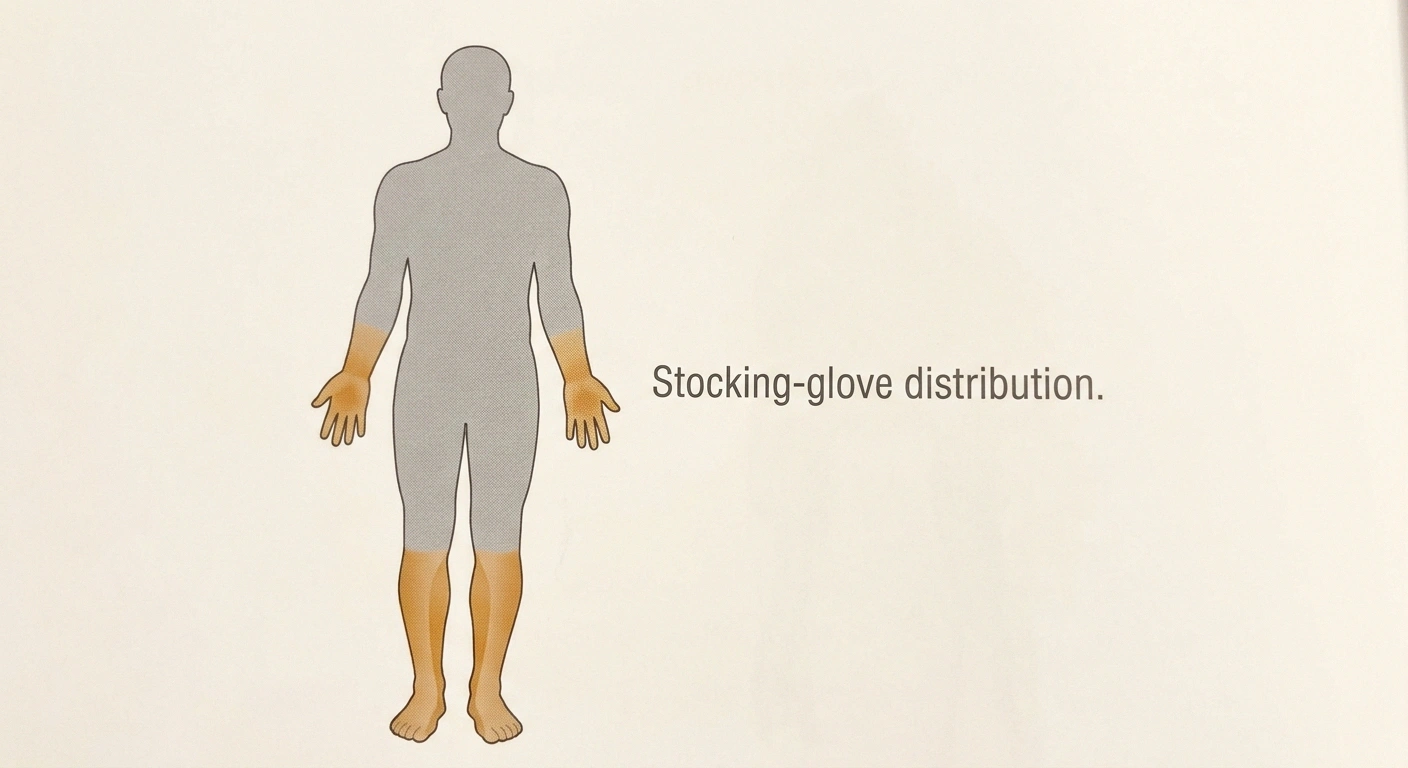
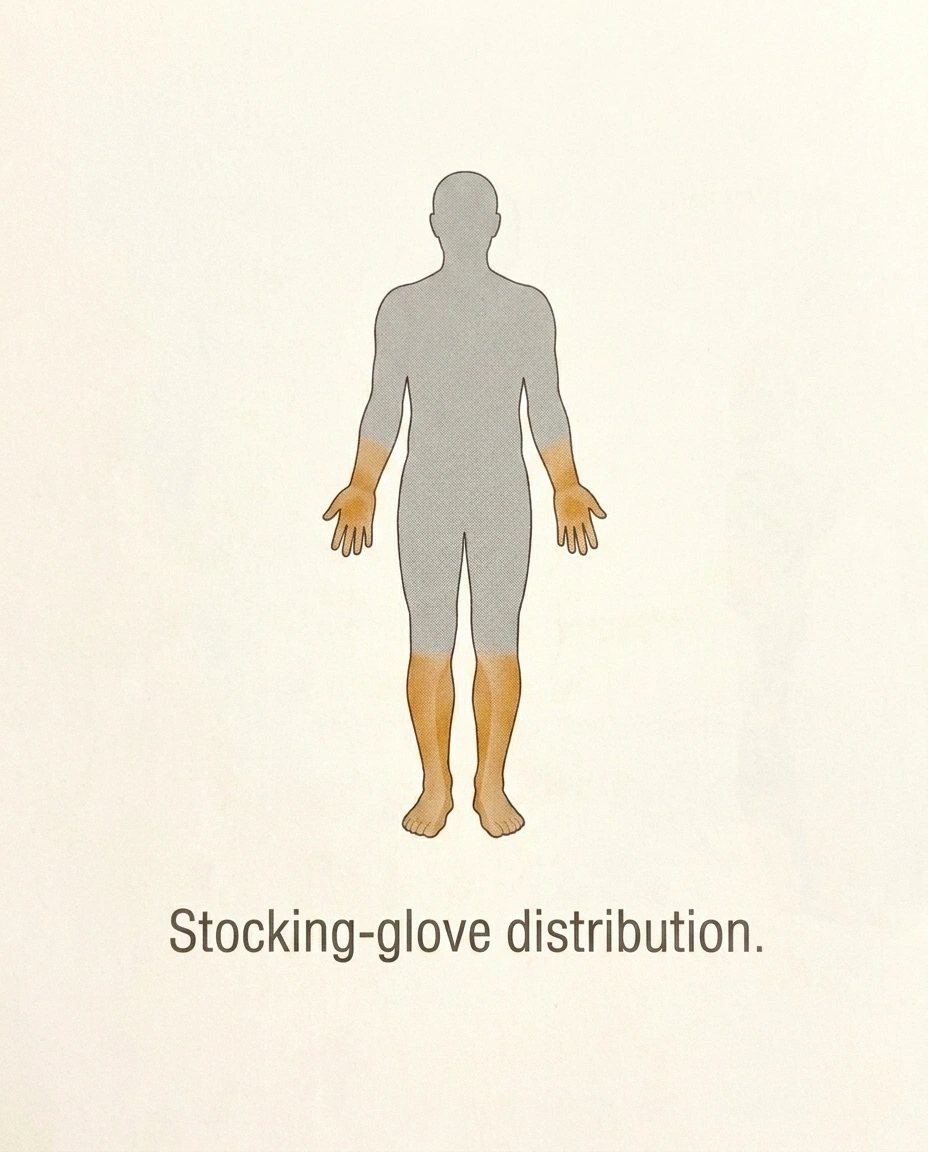
That's why length-dependent neuropathy almost always announces itself in the toes and feet first. Hands, which are served by shorter nerves from the cervical spine, usually don't join in until the leg damage has worked its way up to roughly the mid-calf or knee. The classic term for this pattern is “stocking-glove distribution” — imagine the area of your body covered first by long socks, then later by long gloves. That's the progression.
Why the Longest Nerves Fail First: Five Biological Reasons
It's not arbitrary that long nerves suffer first. Here are the main reasons researchers have identified.
1. The metabolic load is enormous. A neuron has to keep its entire axon supplied with mitochondria, proteins, and waste-removal machinery. The longer the axon, the more of this “housekeeping” has to happen every minute. Any condition that reduces the cell's overall metabolic reserve — diabetes, alcohol toxicity, B-vitamin deficiency — hits the longest, most expensive axons first.
2. Axonal transport has to travel farther. Think of it like a supply truck. Nutrients, structural proteins, and mitochondria travel down the axon from the cell body. In a one-meter axon, that supply line is long and easily disrupted. If the “trucks” are even slightly slow or damaged, the tips don't get their shipments.
3. Blood supply is thinnest at the distal end. Nerves are fed by tiny vessels called the vasa nervorum. The microvasculature that serves the feet is more fragile and more easily damaged than the vessels serving more central structures. Conditions like diabetes that damage small blood vessels worsen this problem dramatically.
4. Your feet are the coldest part of your body. Reduced perfusion and exposure to temperature extremes both add stress to distal nerves. This is one reason many people notice their neuropathy symptoms get worse in cold weather.
5. Daily mechanical stress. Your feet carry your weight all day. That adds physical and microvascular stress no other nerve territory has to endure. Combine it with the four factors above, and distal failure is almost predictable.
When I first understood this, my illness stopped feeling random. It had a reason. My feet weren't unlucky — they were simply the canaries in the coal mine for whatever was happening in my whole nervous system.
The Classic Progression Timeline
Length-dependent neuropathy has a typical order of events. Not everyone follows it exactly, but the general pattern looks like this:
Stage 1 — Toes and balls of feet. Tingling, burning, pins-and-needles, sometimes numbness. Usually symmetric (both feet, not one). Often worse at night.
Stage 2 — Whole feet and lower ankles. Symptoms fill in up to the ankle. Balance may start to feel subtly off, especially in the dark or with eyes closed.
Stage 3 — Up to the mid-calf. The “sock” gets longer. Sometimes weakness appears, especially in the small muscles of the foot. Toes may curl or feel harder to move.
Stage 4 — Fingertips begin. Once leg involvement reaches approximately the knee, the hands typically join in — starting in the fingertips. This is the “glove” forming.
Stage 5 — Whole hands and higher legs. Full stocking-glove distribution. At this stage, autonomic symptoms (digestive changes, blood pressure, sweating irregularities) may also appear if the damage is affecting small autonomic fibers.
This progression can take years or decades, depending on the cause and how well it's being treated. For a more structured view of how neurologists grade severity, I've written about the stages of neuropathy separately.
What's Causing the Damage? The Toxic/Metabolic Pattern
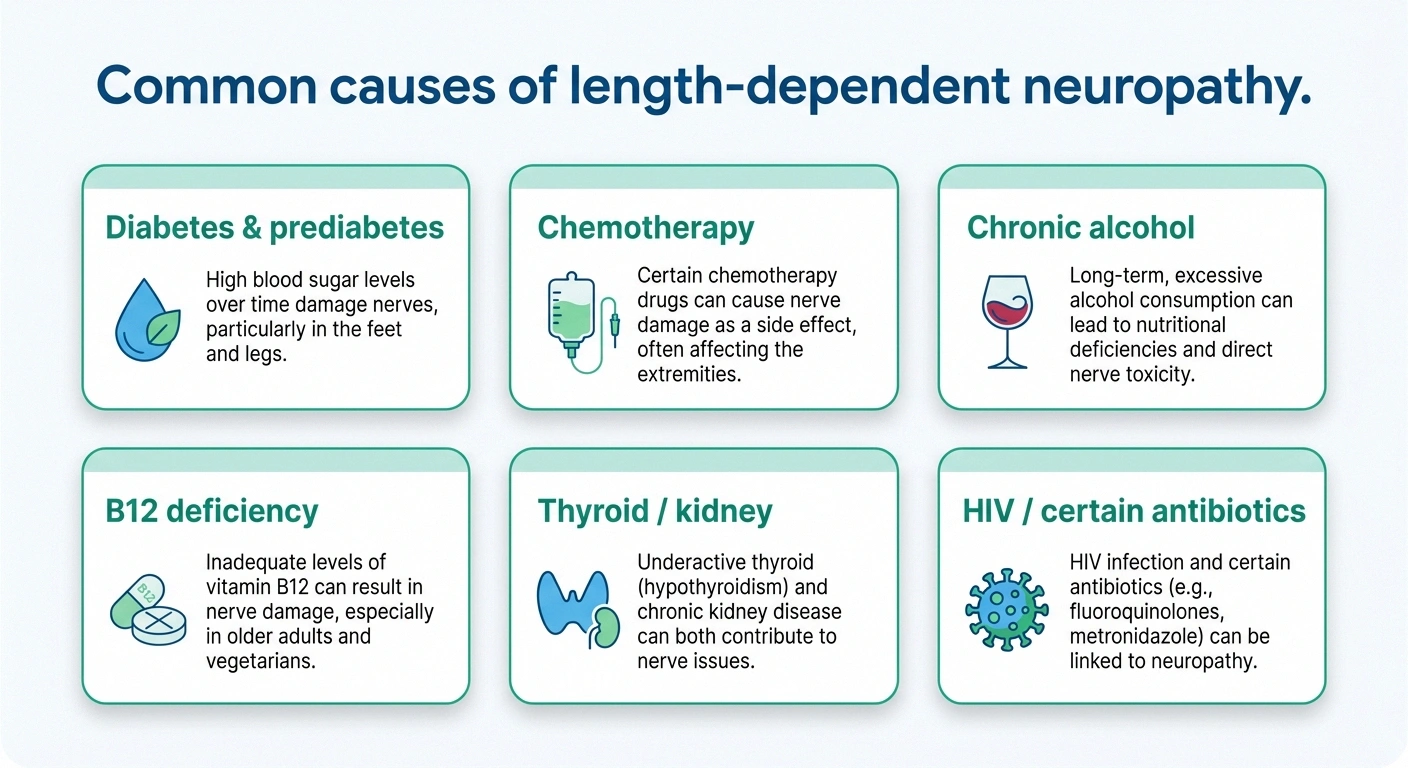
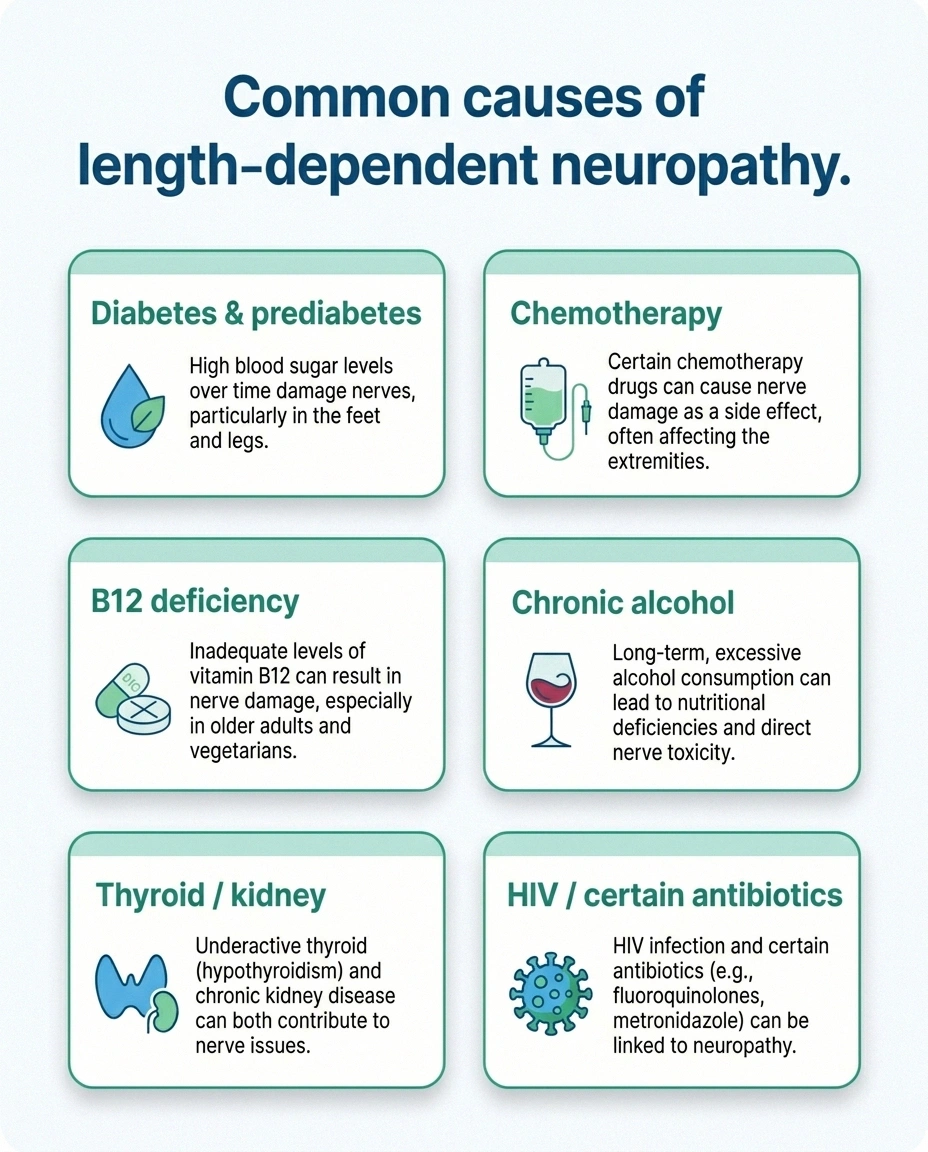
Length-dependent neuropathy has a pretty specific differential diagnosis. Most cases come from a category researchers call “toxic or metabolic” — meaning something in the body's chemistry is wearing down the long nerves over time. The most common culprits:
- Diabetes and prediabetes. By far the leading cause globally. High blood sugar damages the vasa nervorum and disrupts axonal metabolism. Diabetic neuropathy is the textbook example of length-dependent axonopathy.
- Chemotherapy. Platinum drugs, taxanes, and vinca alkaloids are notorious for producing length-dependent sensory damage that often persists after treatment ends.
- Chronic alcohol use. Both a direct toxic effect and a nutritional one (alcohol depletes B vitamins).
- Vitamin B12, B1, and B6 deficiency. Especially B12 — often from pernicious anemia, long-term metformin use, or a strict plant-based diet without supplementation.
- Thyroid disease (particularly hypothyroid).
- Chronic kidney disease (uremic neuropathy).
- HIV (especially untreated) and certain antivirals.
- Certain antibiotics such as fluoroquinolones and metronidazole.
- Autoimmune small-fiber neuropathy. When the immune system targets small unmyelinated fibers, often without a clear trigger.
If you're still working through a diagnosis, our overview of how neuropathy is diagnosed covers the tests a neurologist usually orders to narrow the list.
Red Flags: When the Pattern Isn't Length-Dependent

This is important. A length-dependent pattern — symmetric, feet first, slowly ascending — is actually reassuring in a certain sense. It points toward the common toxic/metabolic causes listed above. When the pattern breaks that rule, neurologists pay closer attention because it can suggest a different, sometimes more urgent, category of nerve damage.
Tell your doctor immediately if you notice:
- Rapid progression — weakness or sensory changes that escalate over days or weeks rather than months or years. This can suggest Guillain-Barré or CIDP.
- Asymmetry — one foot clearly worse than the other, or one hand but not the other. Asymmetric patterns can point to nerve compression or mononeuropathy multiplex.
- Proximal weakness first — trouble climbing stairs, getting out of a chair, or lifting a glass before your feet feel anything. This is not length-dependent and needs workup.
- Hands before feet — genuinely starting in the hands with no foot involvement. Usually points to cervical causes, CTS (carpal tunnel), or cervical radiculopathy.
- Face, tongue, or trunk involvement early — suggests a ganglionopathy or a non-length-dependent pattern.
- Bowel or bladder changes — especially with back pain. Needs urgent evaluation for spinal causes.
If you're ever unsure whether what you're feeling matches the length-dependent pattern, our article on neuropathy emergency signs covers the symptoms that warrant the ER rather than a next-week clinic visit.
Small Fiber vs. Large Fiber — Another Layer of the Pattern
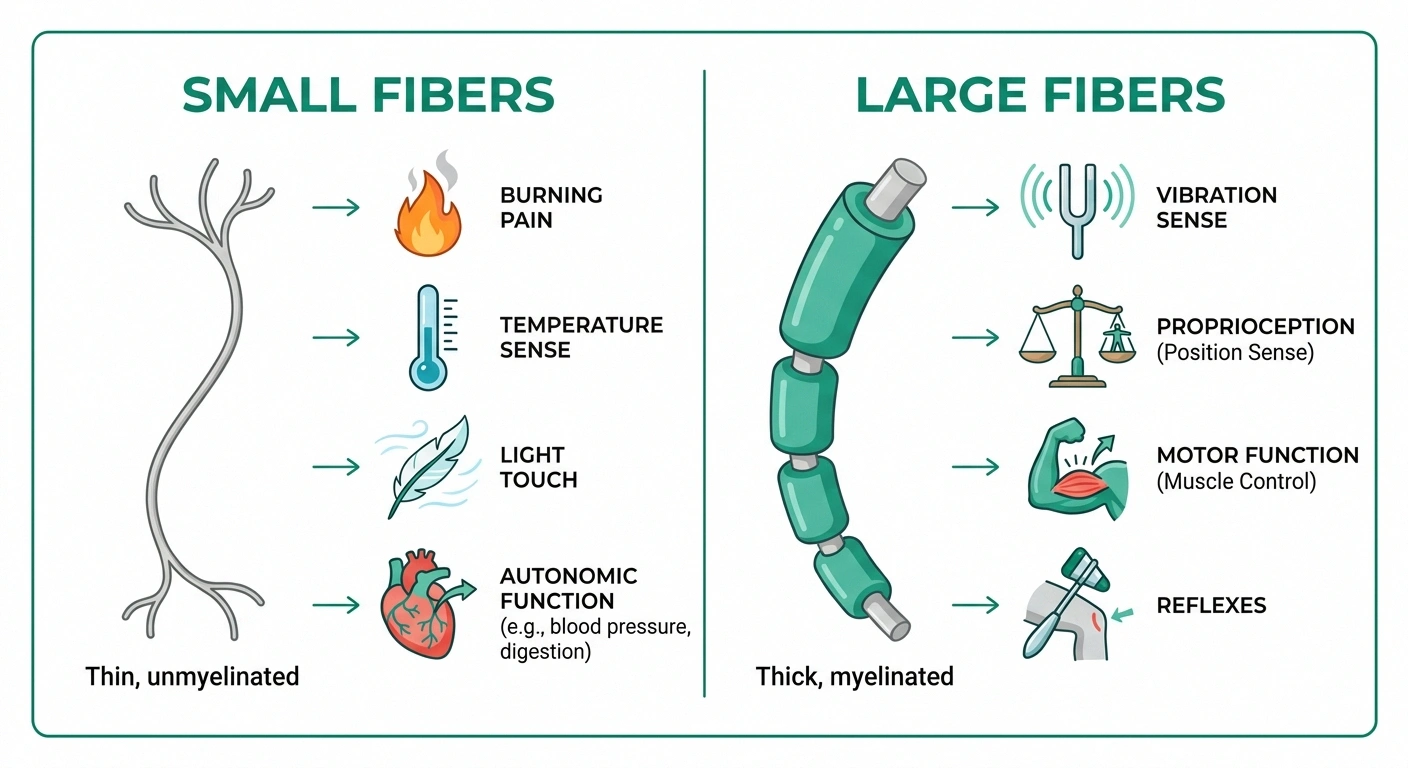
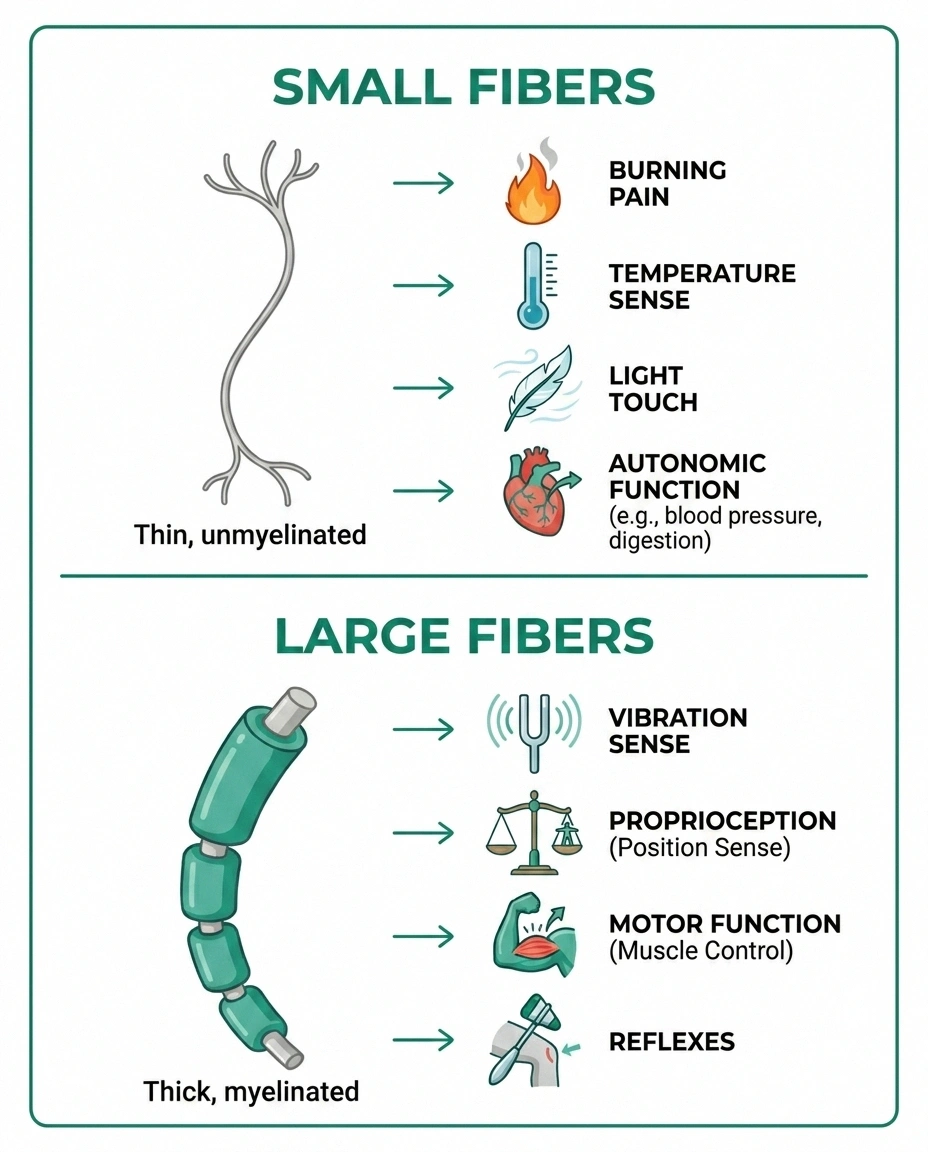
Within length-dependent neuropathy, there's a further distinction that matters for diagnosis and treatment.
- • Burning pain
- • Temperature sensation
- • Light touch
- • Autonomic function
- Often normal on EMG — needs skin biopsy.
- • Vibration sense
- • Proprioception / balance
- • Motor strength
- • Deep tendon reflexes
- Typically picked up by EMG / nerve conduction.
Small fiber symptoms tend to come first in many toxic/metabolic neuropathies. These are the nerves that carry burning, temperature, and light touch, along with autonomic signals. Early symptoms: burning feet, temperature insensitivity, hot/cold feeling reversed, pins-and-needles. Standard EMG and nerve conduction studies can be normal in pure small-fiber damage — which is why patients often feel dismissed. A skin punch biopsy measuring intraepidermal nerve fiber density is the gold-standard test. Our piece on small fiber neuropathy goes into this in depth.
- ⚠Rapid progression over days or weeks (not months)
- ⚠Asymmetry — one side clearly worse than the other
- ⚠Proximal weakness first — stairs, chair rising, lifting
- ⚠Hands before feet with no foot involvement
- ⚠Face, tongue, or trunk symptoms early in the course
- ⚠Bowel or bladder changes with back pain
Large fiber symptoms usually follow. These nerves carry vibration sense, proprioception (knowing where your foot is in space), and motor control. Symptoms: loss of vibration sense in the toes, balance problems, weakness, loss of ankle reflexes. Standard nerve conduction studies are more likely to pick these up.
Many patients have a mixed pattern — both fiber types involved — but the small-fiber symptoms usually appear first. If you've been told your nerve conduction studies are “normal” but your symptoms are real, a skin biopsy is often the next step.
What the Pattern Means for Treatment
Once a length-dependent pattern is confirmed, treatment works on two tracks.
Track 1: Treat the underlying cause. Tight blood-sugar control for diabetes. Replacing B12 if deficient. Stopping or reducing the offending drug when possible. Managing thyroid or kidney disease. This is where the biggest long-term gains come from — you're trying to stop the damage from progressing further.
Track 2: Manage the symptoms. Nerve pain medications (gabapentin, pregabalin, duloxetine, amitriptyline), topical agents (capsaicin cream, lidocaine patches), physical therapy for balance, supplements with evidence (alpha-lipoic acid, benfotiamine, B12), and lifestyle measures.
One thing I want to emphasize: length-dependent neuropathy tends to progress slowly, which means early intervention matters. The damage you prevent today is damage you won't have to live with in five years. If your blood sugar is running high, if your B12 is low, if alcohol is in the picture — these are all modifiable, and the nerves have some capacity to recover when the underlying insult is removed.
Can a Length-Dependent Pattern Reverse?
This is the question I get most often. The honest answer: it depends on what caused it and how long it's been going on.
Small fibers have limited but real regenerative capacity. If the underlying cause is reversed early — blood sugar controlled, B12 replaced, alcohol stopped — many patients see partial symptom improvement over 12 to 24 months. The burning often calms first. Sensation may return gradually to the mid-foot before the toes.
Large fiber axons regenerate at roughly one millimeter per day when the underlying condition is resolved — which sounds slow, but over a year that's almost 36 centimeters. For shorter segments, genuine recovery is possible.
Advanced, long-standing damage is harder to reverse. Axons that have been dying back for a decade may not recover fully, and the longer-standing the damage, the more symptom management becomes the goal rather than reversal. But even in advanced cases, stopping progression is itself a win — it's often the difference between walking and not walking in five years. More on this question in our piece on whether neuropathy can be reversed.
Living With a Length-Dependent Pattern

Because the pattern starts in the feet and slowly ascends, certain practical adaptations help most patients.
- ✓Inspect your feet visually each morning — 5 seconds
- ✓Wear supportive shoes with a wide toe box
- ✓Balance exercise (or walking) daily
- ✓Track how high the symptoms reach once a year
- ✓Stay on top of the metabolic cause — A1C, B12, thyroid
Inspect your feet daily. When sensation is reduced, you can develop blisters, cuts, and infections without feeling them. A five-second visual check every morning prevents small problems from becoming foot ulcers.
Invest in the right shoes and socks. Good cushioning, wide toe boxes, seamless socks. Our article on best shoes for neuropathy covers the specifics.
Address balance early. Length-dependent patterns cause proprioception loss over time. Balance exercises, a consistent walking practice, and removal of home fall hazards all help. Fall prevention is one of the most important investments you can make.
Track your progression. Once a year, map out how high the symptoms reach. If the “sock” is climbing fast, that's useful information for your neurologist.
Stay ahead of the metabolic cause. If diabetes, prediabetes, or B12 is the driver, treat it like a part-time job. Every A1C point matters. Every B12 check matters.
A Final Thought
When I first heard “length-dependent neuropathy,” it sounded like a sentence. Understanding the mechanism turned it into a map. Once you can see the pattern your own illness is following, you can read what the next step is likely to be, catch red flags early, and aim your treatment at the right target.
Your feet went first because they have the longest nerves, not because something about you failed. The damage isn't arbitrary. And in many cases, it's more treatable than you've been told — especially when you catch the cause and act on it.
Frequently Asked Questions
Why does neuropathy almost always start in the feet?
Because your feet are served by the longest peripheral nerves in your body — almost a meter of axon from the lumbar spine to the toes. Longer axons have higher metabolic demands, more fragile distal blood supply, and more vulnerable axonal transport. When the cell body has to support a very long wire, the tip fails first. This is the essence of a length-dependent or “dying-back” neuropathy.
What is the stocking-glove distribution?
It's the classic visual pattern of length-dependent neuropathy. Symptoms start in the toes and ascend up the feet and legs like a sock being pulled on. Only after the leg symptoms reach approximately the mid-calf or knee do the hands and fingers usually begin to show symptoms — the “glove.” The pattern is symmetric, meaning both sides of the body are affected roughly equally.
When do the hands usually start being affected in length-dependent neuropathy?
Typically only after the leg involvement has climbed to about the mid-calf or knee level. That's because the nerves serving the hands are shorter than the nerves serving the feet, so they're more resistant to length-dependent damage. If your hands feel affected before your feet have reached the knee, tell your neurologist — it may suggest a non-length-dependent cause that needs a different workup.
What's the difference between length-dependent and non-length-dependent neuropathy?
Length-dependent neuropathy is symmetric, starts distally (feet first), and ascends gradually. It usually reflects a toxic or metabolic cause like diabetes, chemotherapy, B12 deficiency, or alcohol. Non-length-dependent neuropathy can start anywhere, can be asymmetric, and can involve the hands, trunk, or face early. It often points to immune, infectious, or ganglionopathic causes and generally warrants a more aggressive diagnostic workup.
What are the most common causes of length-dependent neuropathy?
Diabetes and prediabetes are the leading causes worldwide. Other common contributors include chemotherapy, chronic alcohol use, B12 deficiency, thyroid disease, chronic kidney disease, HIV, certain antibiotics, and idiopathic or immune small-fiber neuropathy. In some cases, no cause is found despite thorough testing, which is called idiopathic neuropathy.
Can a length-dependent neuropathy be reversed?
Partial reversal is possible, especially when the underlying cause is treated early. Small fibers have some regenerative capacity and large fiber axons can regrow at roughly one millimeter per day. Patients who control blood sugar tightly, correct B12 deficiency, or stop alcohol often see measurable improvement over 12 to 24 months. Long-standing, advanced damage may not fully reverse, but stopping progression is itself a meaningful outcome.
Why were my nerve conduction studies normal when my symptoms are obviously real?
Standard nerve conduction studies measure large myelinated fibers. Many length-dependent neuropathies begin in small unmyelinated fibers, which don't show up on these tests. If you have classic burning, temperature, or autonomic symptoms but normal nerve conduction, ask about a skin punch biopsy measuring intraepidermal nerve fiber density. That's the gold standard for diagnosing small fiber neuropathy.
How fast does length-dependent neuropathy usually progress?
Usually slowly — over months to years — which is one of its reassuring features. Rapid progression over days or weeks is a red flag and suggests a different, often urgent cause such as Guillain-Barré syndrome, CIDP, or vasculitic neuropathy. If your symptoms are ascending quickly, treat that as a reason to be seen sooner rather than later.