Of all the things I've had to learn living with neuropathy, the one that took the longest to wrap my head around is this: my own immune system — the thing that fights infections and patches wounds — can be the source of nerve damage. The body that's supposed to protect me can also misfire and start attacking the wires that carry sensation and movement.
If you've been told your neuropathy is “autoimmune” or “immune-mediated,” or if your doctor has used the word “idiopathic” and you've started to wonder whether something deeper is going on, this guide is for you. We're going to walk through what autoimmunity actually means, the specific ways the immune system damages nerves, why type matters, and the conversation worth having with your neurologist if you suspect immune involvement. None of this is a substitute for testing — but knowing the landscape changes the questions you can ask.
What “Autoimmune Neuropathy” Actually Means
The immune system has one main job: tell the difference between “you” and “not you.” When it works well, it attacks invading bacteria, viruses, and damaged cells while leaving the rest of your body alone. The mechanism it uses to do this is called self-tolerance. Healthy immune cells are trained, early in life, not to react to your own tissues.
An autoimmune disease is what happens when self-tolerance breaks down. The immune system mistakes part of you for an invader and attacks it. Lupus attacks joints, skin, kidneys. Type 1 diabetes attacks insulin-producing cells. Multiple sclerosis attacks the myelin in the brain and spinal cord.
Autoimmune neuropathy is the same problem, aimed at your peripheral nerves — the wires that carry signals between the spinal cord and the rest of the body. Different conditions attack different parts of those wires, which is why the symptoms vary so much from one autoimmune neuropathy to another.
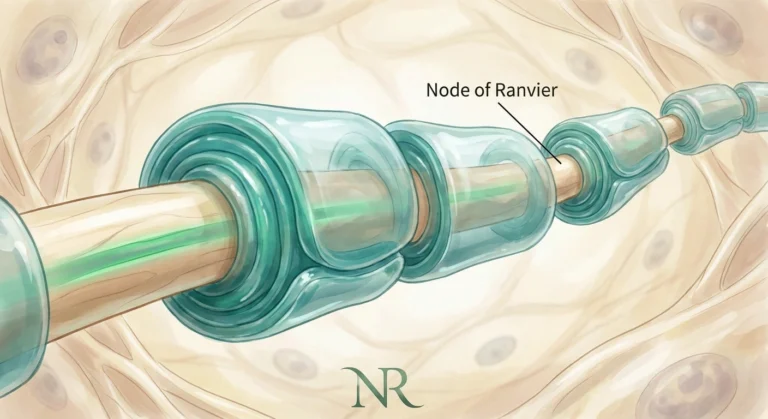
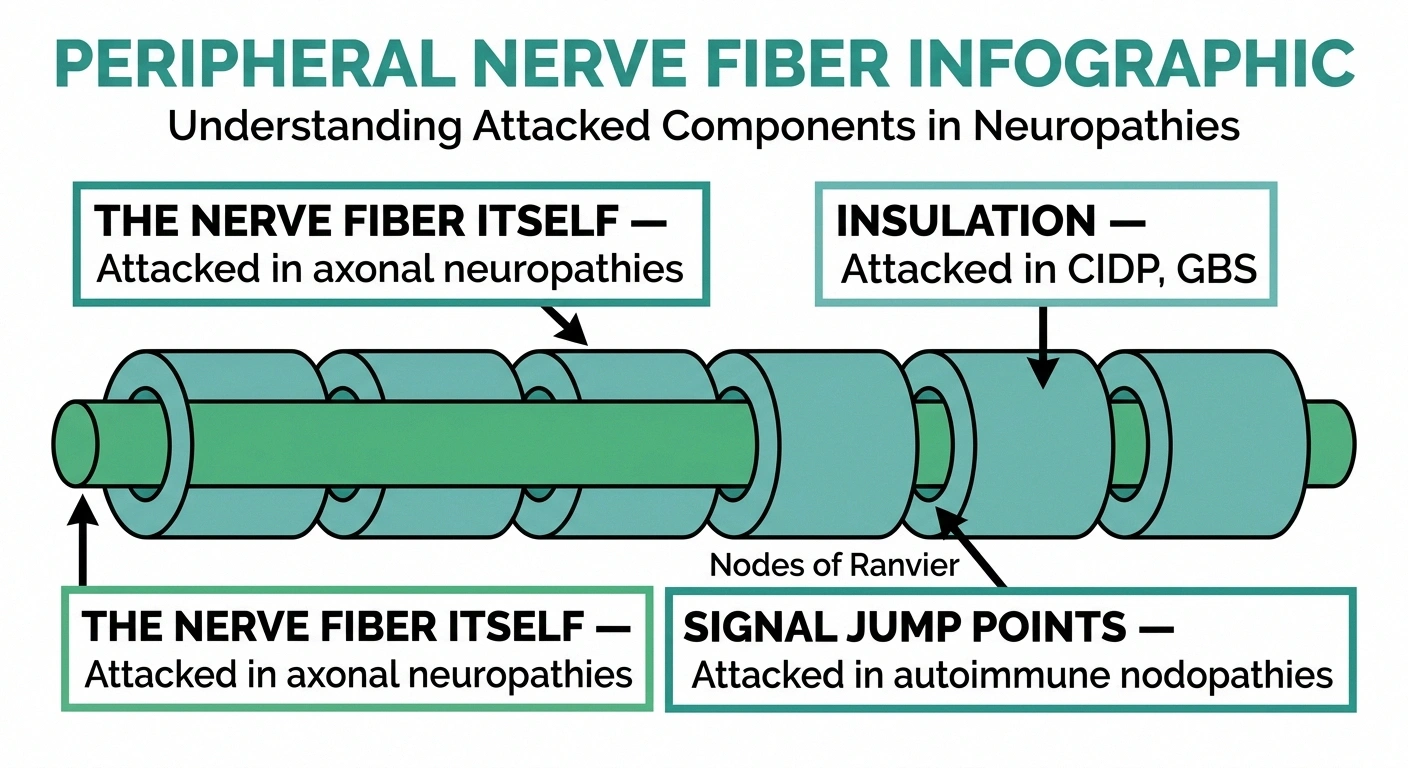
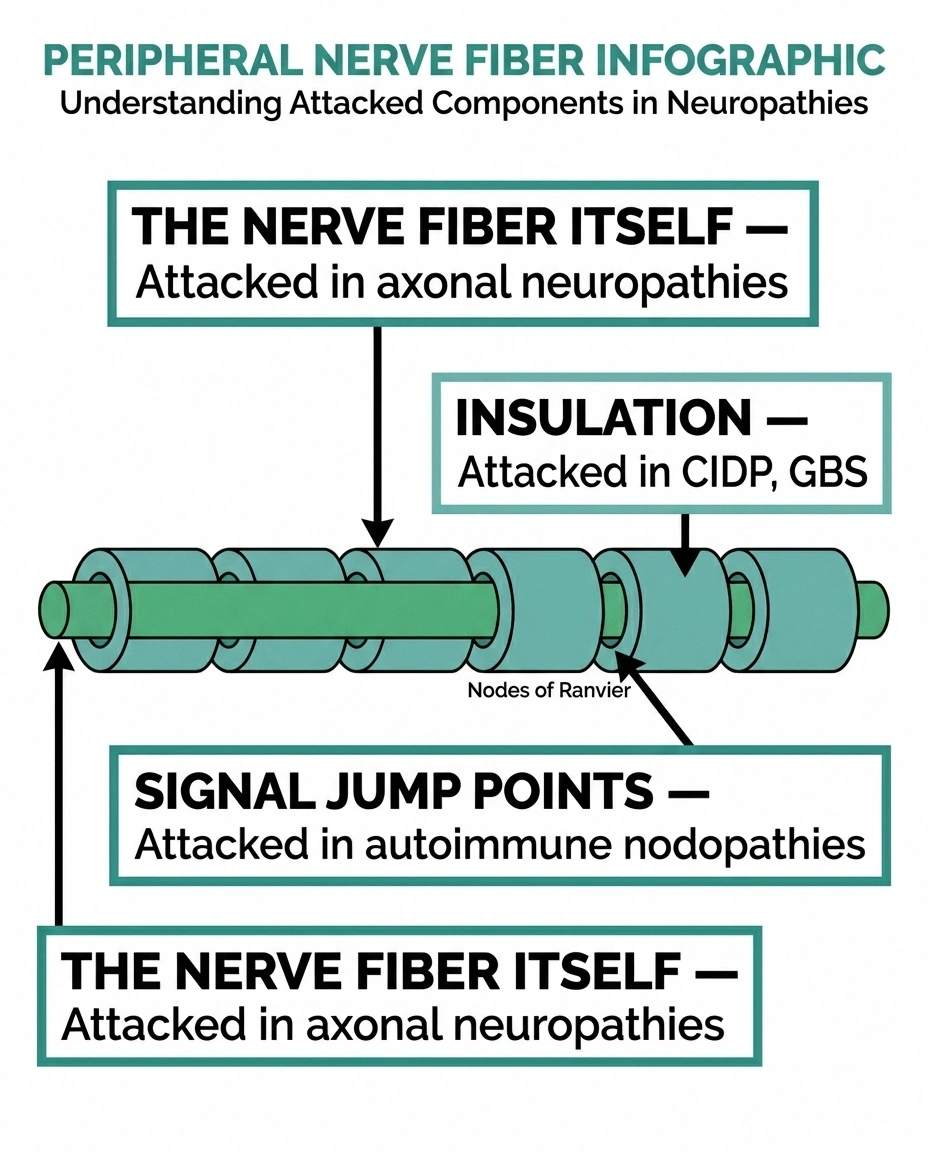
The peripheral nerve has three main parts the immune system can target:
- The myelin sheath — the fatty insulation wrapped around the nerve fiber that lets signals travel fast.
- The axon — the wire itself, the long extension of the nerve cell that carries the electrical signal.
- The nodes of Ranvier — the small gaps between segments of myelin where signals “jump” along the nerve.
Damage in different locations causes different symptom patterns and responds to different treatments. This is why diagnosing the specific subtype matters so much.
Key Takeaway
Autoimmune neuropathy is your immune system attacking your own nerves — the myelin insulation, the nerve fiber itself, or the nodes between segments. Different targets cause different symptoms and respond to different treatments. Knowing the precise subtype is what unlocks the right care.
How the Immune System Damages a Nerve
There are two main ways the immune system causes nerve damage. Most autoimmune neuropathies use both, in varying proportions.
Two Ways the Immune System Damages Nerves
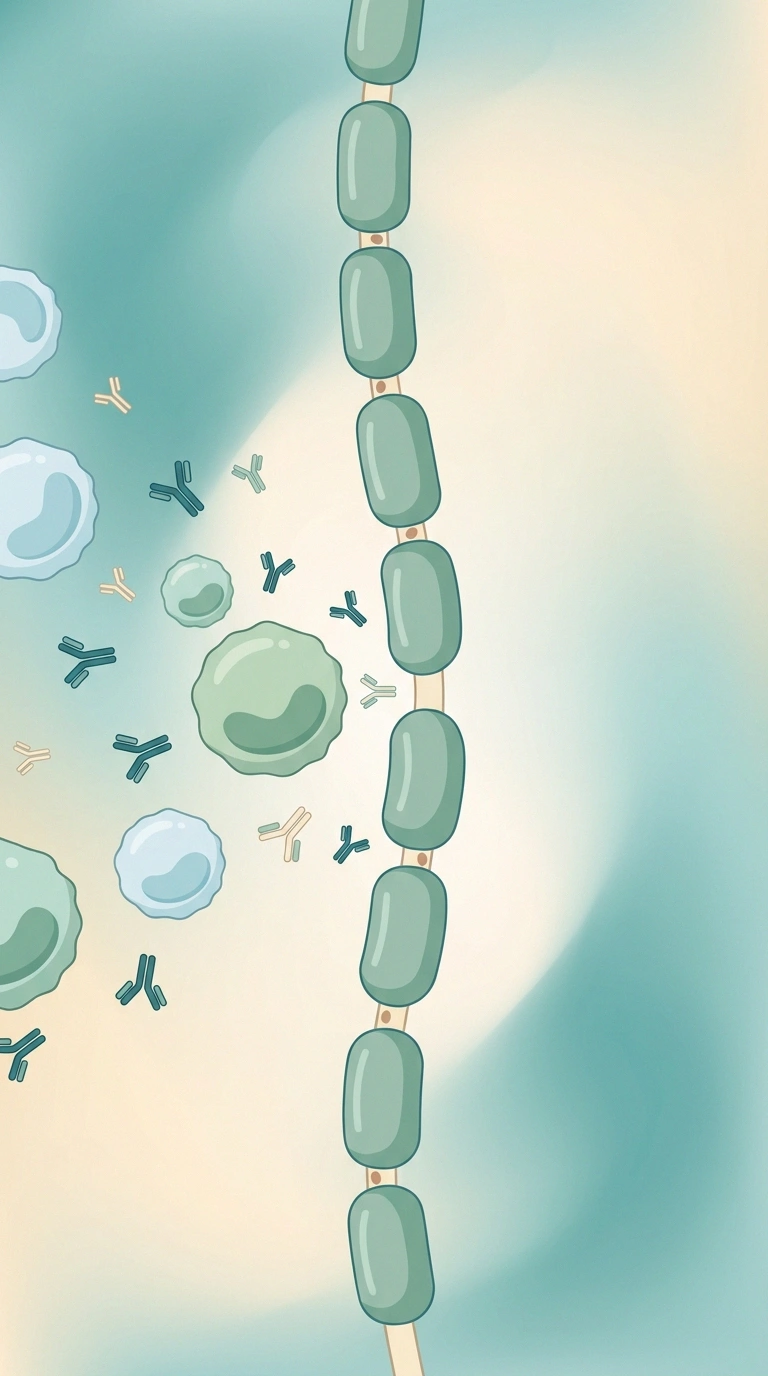
1. Antibody-Driven (Humoral)
The immune system makes antibodies that mistakenly tag your own myelin, axonal proteins, or nodal proteins. Once tagged, the nerve is attacked by complement and other immune cells. This is the mechanism behind autoimmune nodopathies and anti-MAG neuropathy.
2. Cell-Driven (Cellular)
T-cells and macrophages infiltrate the nerve directly, stripping myelin and damaging the axon. Macrophage infiltration is a hallmark of CIDP and Guillain-Barré.
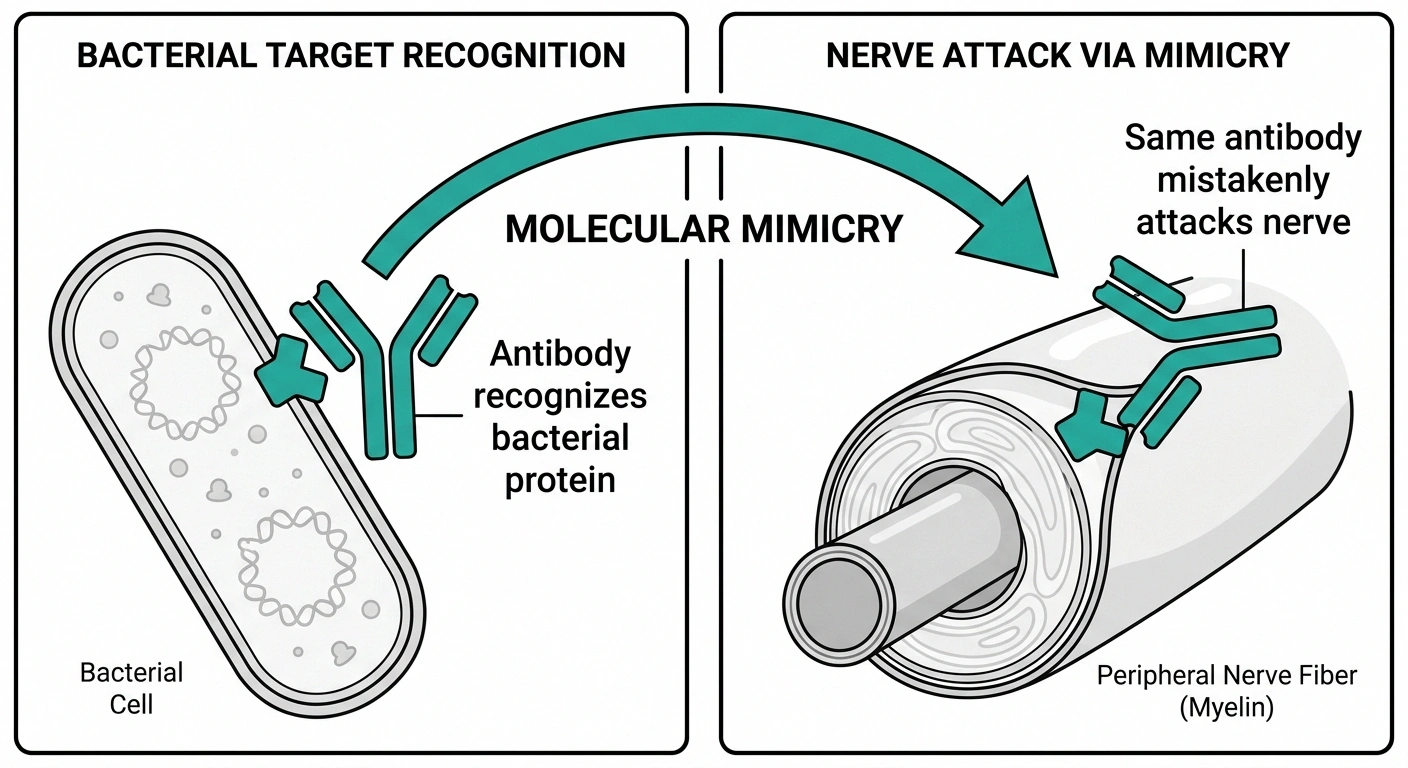
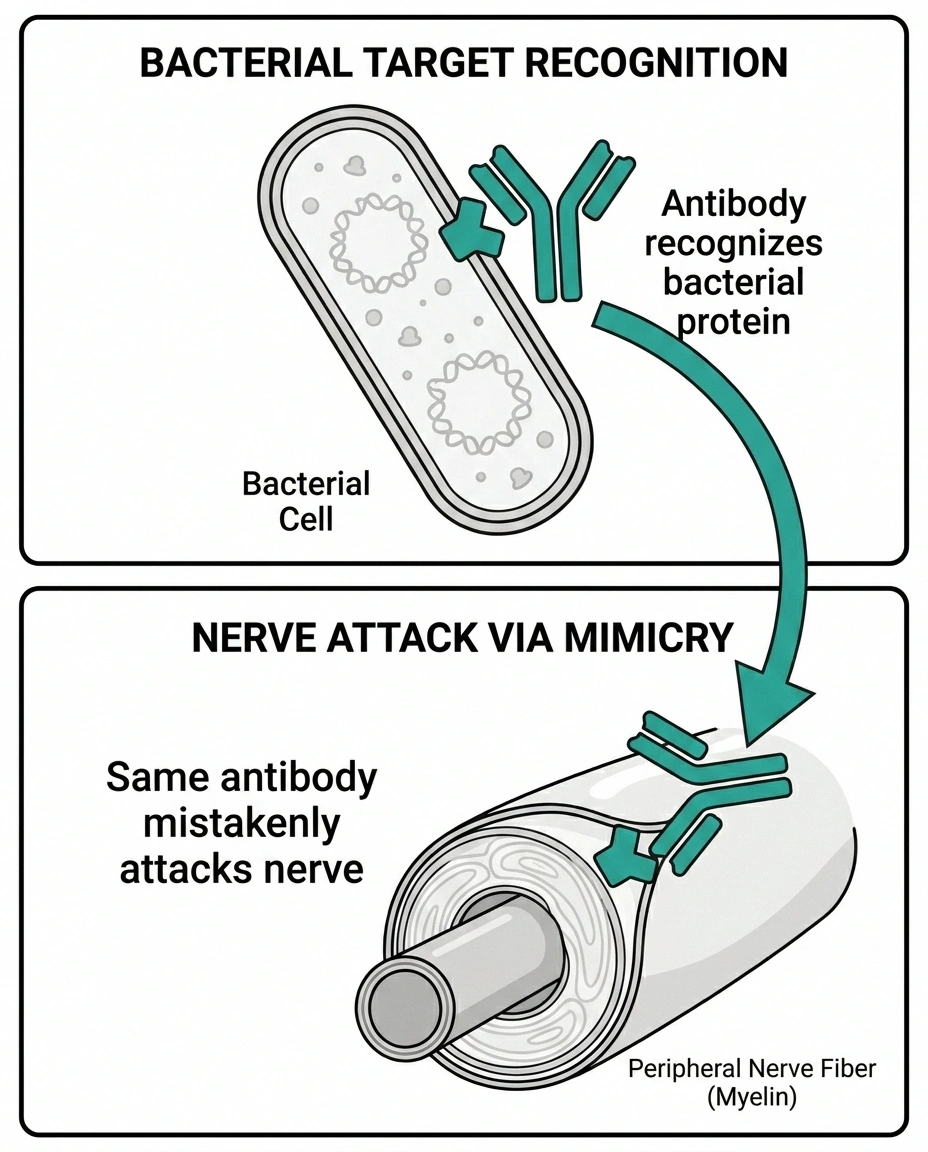
Molecular Mimicry: Why It Often Starts After Infection
A protein on a virus or bacteria looks similar enough to a nerve protein that antibodies made to fight the infection cross-react with your own nerves. This is why Campylobacter gastroenteritis is the classic trigger for Guillain-Barré syndrome.
Antibody-driven (humoral) attack. Your immune system makes proteins called antibodies that normally tag invaders for destruction. In autoimmune neuropathy, antibodies form against components of your own nerves — myelin proteins, axonal proteins, or proteins at the nodes. Once tagged, the nerve gets attacked by other immune cells and the complement system (a cascade of proteins that punches holes in cell membranes).
Cell-driven (cellular) attack. White blood cells, particularly T-cells and macrophages, infiltrate the nerve directly. Macrophages are the immune system's clean-up crew — they engulf and digest tissue. When pointed at nerves, they strip away myelin and damage the underlying axon.
One concept worth understanding is molecular mimicry. Some autoimmune neuropathies start when you fight off an infection, and a protein on the bacteria or virus happens to look similar to a protein on your own nerves. The antibodies your immune system made to fight the infection cross-react with your nerves and start attacking them. This is the mechanism behind the classic Guillain-Barré syndrome that follows a Campylobacter gastrointestinal infection — the bacterial protein resembles a nerve protein closely enough that the antibodies don't tell them apart.
Once started, the attack can be self-sustaining. Damaged nerve releases more proteins into the bloodstream, the immune system sees them as foreign, and the cycle continues. This is why immune-modulating treatment — interrupting the attack — is often more effective than just treating symptoms.
The Major Autoimmune Neuropathies
Several distinct conditions fall under the autoimmune neuropathy umbrella. They differ by speed of onset, what part of the nerve is attacked, what antibodies are involved, and what treatments work best.
Major Autoimmune Neuropathies at a Glance
| Condition | Speed | Target | First-Line Treatment |
|---|---|---|---|
| Guillain-Barré (GBS) | Acute (days–weeks) | Myelin (motor mostly) | IVIG or plasma exchange |
| CIDP | Chronic (8+ weeks) | Myelin | Steroids, IVIG, plasma exchange |
| MMN | Slow, progressive | Motor nerves only | IVIG (steroids don't work) |
| Vasculitic Neuropathy | Subacute, asymmetric | Nerve blood supply | High-dose immunosuppression |
| Autoimmune Nodopathies | Looks like CIDP | Nodes of Ranvier | Rituximab (B-cell depletion) |
| Anti-MAG Neuropathy | Slow (sensory&dominated) | Myelin (sensory) | Rituximab, IVIG variable |
Guillain-Barré Syndrome (GBS). The acute, fast version. GBS develops over days to a few weeks, often two to three weeks after an infection. Weakness starts in the legs and ascends — feet to legs to arms to face. About 70 percent of cases follow an identifiable infection (Campylobacter, flu, COVID-19, EBV). It's a medical emergency: people can lose the ability to walk, and severe cases affect breathing. With IVIG or plasma exchange, most people recover, but recovery can take months and a portion are left with lingering deficits. Read more in our complete guide to Guillain-Barré syndrome.
Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP). The slow version. CIDP is essentially GBS that doesn't end — the immune attack on myelin keeps going for months and years. Symptoms develop over at least eight weeks, often longer. Weakness, numbness, and reduced reflexes affect both arms and legs symmetrically. CIDP is treatable with corticosteroids, IVIG, or plasma exchange. Some patients respond to one treatment but not another, which is part of why getting the diagnosis precisely right matters. See our deep-dive on CIDP.
Multifocal Motor Neuropathy (MMN). A rarer cousin of CIDP that affects only motor nerves (movement, not sensation). Hand and arm weakness is usually the first symptom — a grip that gradually fails. People are sometimes misdiagnosed with ALS until antibody testing or nerve conduction studies clarify the picture. MMN responds well to IVIG but typically not to corticosteroids.
Vasculitic Neuropathy. Inflammation of the small blood vessels supplying the nerves cuts off the blood supply, causing nerve infarction. Symptoms tend to be patchy and asymmetric — pain and numbness in one foot, then a hand, in a “stepwise” pattern called mononeuritis multiplex. Vasculitic neuropathy is associated with conditions like polyarteritis nodosa, granulomatosis with polyangiitis, and rheumatoid vasculitis. It's a medical emergency requiring high-dose immunosuppression.
Autoimmune Nodopathies. A newly defined category, formally separated from CIDP within the last few years. People with these conditions have antibodies against proteins at the nodes of Ranvier — anti-neurofascin 155, anti-contactin 1, anti-CASPR1. They look like CIDP on first glance but often don't respond to standard CIDP treatments. They do respond to rituximab, which targets the B-cells that make the offending antibodies. This is one of the most important recent diagnostic advances and a strong argument for getting full antibody testing if your “CIDP” isn't responding to expected treatments.
Anti-MAG Neuropathy. A slowly progressive neuropathy associated with an abnormal antibody called anti-MAG (myelin-associated glycoprotein). Symptoms are predominantly sensory — numbness, tingling, balance problems — with relatively preserved strength. It's associated with a blood disorder called IgM monoclonal gammopathy.
When Neuropathy Comes with Another Autoimmune Disease
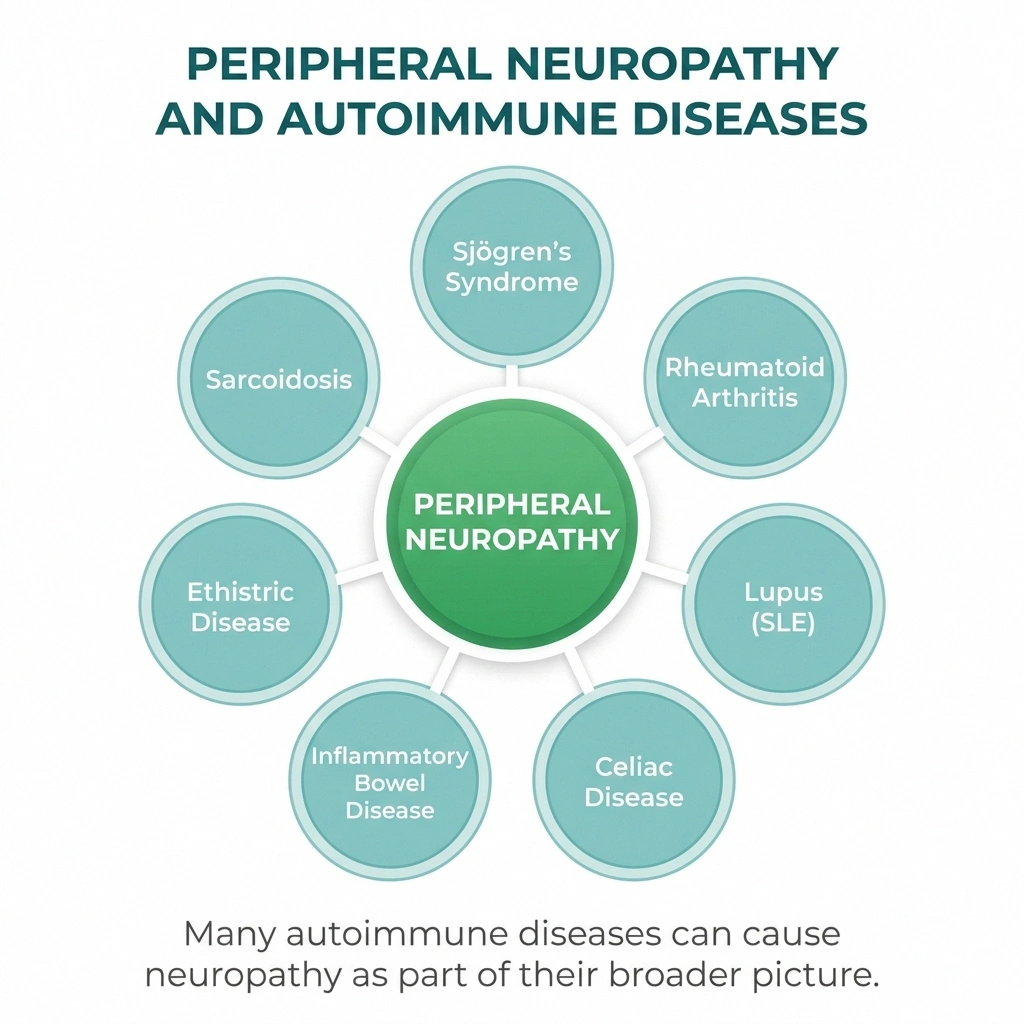
Sometimes the immune system attacks your nerves as part of a broader autoimmune condition. If you already have one of these diagnoses, neuropathy isn't a separate problem — it's part of the same disease, and treating the underlying condition often improves the nerve symptoms.
Research Says
A 2025 Nature Reviews Neurology review on the changing landscape of primary autoimmune neuropathies described autoimmune nodopathies as a newly defined diagnostic category. Patients previously labeled with “treatment-resistant CIDP” who carry anti-neurofascin 155, anti-contactin 1, or anti-CASPR1 antibodies often respond to rituximab when standard CIDP treatments have failed. This is one of the strongest current arguments for full antibody panels in atypical cases.
- Sjögren's syndrome. The autoimmune condition that causes dry eyes and dry mouth also causes neuropathy in roughly 10 to 60 percent of patients depending on how it's measured. Small fiber neuropathy and sensory ataxia are the most common forms. Sjögren's-related neuropathy is one of the most under-diagnosed causes of “idiopathic” sensory neuropathy.
- Rheumatoid arthritis. Affects nerves through compression (joint swelling pinching nearby nerves), through medication side effects, and occasionally through vasculitic neuropathy.
- Lupus (SLE). Can cause peripheral neuropathy through several mechanisms — vasculitis, autoantibodies, or as a side effect of treatment.
- Celiac disease. A surprisingly common cause of “idiopathic” neuropathy. Some people develop nerve symptoms before any digestive symptoms, and a strict gluten-free diet can resolve or stabilize the neuropathy.
- Inflammatory bowel disease. Both Crohn's and ulcerative colitis are linked to peripheral neuropathy, sometimes through vitamin malabsorption (B12, B6) and sometimes through direct immune mechanisms.
- Sarcoidosis. A granulomatous inflammatory disease that can affect peripheral nerves directly. Sarcoid neuropathy can be small-fiber, large-fiber, or cranial.
- Type 1 diabetes. The damage from diabetic neuropathy is largely metabolic, but the underlying disease — type 1 diabetes — is itself autoimmune (the immune system destroys pancreatic insulin-producing cells).
If you have one of these conditions and you're developing nerve symptoms, talk to the specialist who manages the underlying disease in addition to your neurologist. The two often need to coordinate.
The “Idiopathic” Problem: When Autoimmune Neuropathy Gets Missed

Here's something that doesn't get talked about enough. A meaningful percentage of people diagnosed with idiopathic peripheral neuropathy — meaning “we don't know what's causing it” — actually have an autoimmune cause that wasn't tested for.
“Idiopathic” doesn't mean the cause doesn't exist. It means the workup didn't find one. Standard neuropathy workups often check diabetes, B12, thyroid, alcohol, and a few obvious medications. A thorough autoimmune workup goes further — testing for Sjögren's antibodies, celiac antibodies, ANA (lupus screen), specific paraneoplastic and node-of-Ranvier antibodies, and inflammatory markers. Many neurologists order these, but not all do, and not all order the full panel on first evaluation.
If your neuropathy has any of the following features, an autoimmune workup is worth asking about:
- Symptoms came on relatively quickly (over weeks to months, not years)
- Pattern is asymmetric — one side worse than the other, or patchy across limbs
- You have weakness in addition to sensory symptoms
- You have other autoimmune symptoms (dry eyes, dry mouth, joint pain, rashes, GI issues, fatigue)
- Family history of autoimmune disease
- Symptoms that respond unpredictably — better some weeks, worse others, no clear trigger
- Standard treatments aren't helping
A nerve conduction study showing demyelinating features (slowing of nerve signals, conduction block) is another red flag for an immune-mediated cause and reason to push for antibody testing. The neuropathy diagnosis guide walks through what tests are typically ordered and which ones to specifically ask for if autoimmune is on the table.
Treatments That Target the Immune System

Standard neuropathy medications — gabapentin, pregabalin, duloxetine, tricyclics — treat the pain signal, not the cause. They don't change what your immune system is doing. For autoimmune neuropathy, the more important treatments are the ones that calm or modify the immune attack itself.
Immune-Targeted Treatments at a Glance
Corticosteroids (prednisone)
Broad immune suppression. Effective for CIDP and vasculitic neuropathy. Side effects (weight, blood sugar, bone loss) push toward tapering or transitioning to a steroid-sparing agent.
IVIG (Intravenous Immunoglobulin)
Pooled donor antibodies that modulate the immune response. Works for GBS, CIDP, and MMN. Expensive but well-tolerated. Typically every few weeks.
Plasma Exchange (Plasmapheresis)
Filters antibodies out of the blood physically. Effective for GBS and some CIDP. More invasive than IVIG (vascular catheter required) but works through a different mechanism.
Immunosuppressants
Azathioprine, mycophenolate, methotrexate. Steroid-sparing agents for long-term control. Take weeks to work; require regular blood monitoring.
Rituximab (B-cell depletion)
Targets the B-cells that make the offending antibodies. Often works when standard CIDP treatments fail — particularly in autoimmune nodopathies and anti-MAG neuropathy.
Red Flags for an Autoimmune Workup
- Symptoms developed over weeks to months, not years
- Pattern is asymmetric — one side worse than the other, or patchy
- Weakness in addition to sensory symptoms
- Other autoimmune symptoms: dry eyes, dry mouth, joint pain, rashes, GI issues, fatigue
- Family history of autoimmune disease
- Symptoms that fluctuate unpredictably
- Standard neuropathy treatments aren't helping
Action: Ask your neurologist about a full autoimmune panel including Sjögren's antibodies, celiac antibodies, ANA, and node-of-Ranvier antibodies (anti-NF155, anti-CNTN1, anti-CASPR1).
Corticosteroids (prednisone). Broad immune suppression. Effective for CIDP, vasculitic neuropathy, and several other immune neuropathies. Long-term use has significant side effects — weight gain, blood sugar issues, bone loss, mood changes — so the goal is usually to taper to the lowest effective dose or transition to a steroid-sparing immunosuppressant.
IVIG (Intravenous Immunoglobulin). Pooled antibodies from healthy donors, given by infusion. Mechanism isn't fully understood, but IVIG modulates the immune response in ways that often work for GBS, CIDP, and MMN. Treatments are typically every few weeks. Expensive but well-tolerated. Read about what IVIG treatment involves.
Plasma exchange (plasmapheresis). A procedure that removes antibodies from the blood by filtering plasma. Effective for GBS and some CIDP. Requires a vascular catheter and is more invasive than IVIG, but works through a different mechanism — physical antibody removal rather than immune modulation. Read more about plasma exchange for neuropathy.
Immunosuppressants. Drugs like azathioprine, mycophenolate, methotrexate, and cyclophosphamide suppress immune cell production or function. Used as steroid-sparing agents and for treatment-resistant cases. They take weeks to months to show effect and require regular blood monitoring.
Rituximab. A targeted therapy that depletes B-cells (the immune cells that make antibodies). Particularly effective for autoimmune nodopathies and some other antibody-driven neuropathies. It's the treatment that often works when standard CIDP treatments fail.
None of these are casual prescriptions. They all require a neurologist or neuromuscular specialist to manage, and they all involve trade-offs between disease control and side effects. The point is that they exist — and that the right one for your specific neuropathy depends on knowing exactly what kind you have.
Living Well When the Immune System Is the Problem
Living with autoimmune neuropathy is different from living with metabolic neuropathy in one important way: the disease can flare. You can have stretches of relative stability and stretches of active attack. That changes how you plan your life and what to watch for.
Six Anchors for Living with Autoimmune Neuropathy
A few practical anchors I've learned from talking to people in support groups who've navigated this for years:
- Find a neuromuscular specialist, not just a general neurologist. Subspecialists at academic medical centers see more of these conditions and are more likely to test for the less common antibodies and to know which treatments work for which subtypes.
- Get the diagnosis precisely right. “CIDP” or “autoimmune neuropathy” isn't enough. Push for the specific subtype — which antibodies are present, where the damage is on the nerve, what pattern of conduction abnormality you have. The treatment depends on it.
- Track your symptoms. A simple weekly log — pain levels, weakness, balance changes — gives you and your doctor data when you're trying to tell whether a flare is starting or whether a treatment is working.
- Watch for new autoimmune symptoms. If your immune system has misfired once, you're at higher risk of developing other autoimmune conditions. New unexplained joint pain, dry eyes, GI issues, or rashes warrant a conversation with your doctor.
- Be careful with vaccines you don't need but okay with the ones you do. Most autoimmune neuropathy specialists recommend that patients follow standard vaccination schedules — the risk of infection-triggered flares (especially flu and COVID) is generally higher than the very small risk of vaccine-related reactions. But discuss timing of any new vaccine with your specialist.
- Know your treatment escape ladder. If your current immunomodulating treatment stops working, what's next? Your neurologist should be able to walk you through the sequence — IVIG, then plasma exchange, then rituximab, or whichever order fits your subtype. Knowing the ladder reduces the panic when something stops working.
Autoimmune neuropathy is harder to live with in some ways and easier in others. Harder, because the disease can be unpredictable. Easier, because there are real, effective treatments that work on the cause — not just the symptoms — and a specific diagnosis often opens doors that “idiopathic” doesn't. Knowing the immune system is the source isn't bad news. It's actionable news.
Frequently Asked Questions
What does “autoimmune neuropathy” actually mean?
Autoimmune neuropathy means your own immune system has lost the ability to tell the difference between you and a foreign invader, and is attacking your peripheral nerves as if they were a virus or bacteria. The attack can target the myelin sheath around nerves, the nerve fiber itself, or the nodes between segments of myelin. Different targets cause different symptom patterns and respond to different treatments.
How is autoimmune neuropathy diagnosed?
The workup typically includes a nerve conduction study and EMG to characterize the type of damage, blood tests for specific antibodies (anti-ganglioside, anti-MAG, anti-neurofascin, anti-contactin, anti-CASPR1, ANA, Sjögren's antibodies, celiac panel, and others), inflammatory markers, and sometimes a lumbar puncture to look at spinal fluid protein levels. A nerve biopsy is occasionally needed when other tests are inconclusive. A neuromuscular subspecialist is best equipped to order and interpret the right combination.
What's the difference between Guillain-Barré syndrome and CIDP?
Both are immune attacks on the myelin of peripheral nerves, but Guillain-Barré is acute — symptoms develop over days to a few weeks, often after an infection — and is essentially a one-time event. CIDP is chronic — symptoms develop over at least eight weeks and continue or relapse. GBS treatment is short-term (one course of IVIG or plasma exchange). CIDP treatment is ongoing, often for years, with regular IVIG, corticosteroids, or other immunomodulating drugs.
Can autoimmune neuropathy be cured?
“Cure” is a strong word, but Guillain-Barré often resolves with treatment and most patients recover well, though some have lingering deficits. CIDP and the other chronic autoimmune neuropathies aren't cured but can often be put into remission or well-controlled with appropriate treatment. The goal is to interrupt the immune attack and protect the nerves before permanent damage accumulates. Earlier diagnosis and treatment generally lead to better outcomes.
Is “idiopathic” neuropathy actually autoimmune?
Sometimes. “Idiopathic” means the standard workup didn't find a cause. A meaningful percentage of these cases turn out to have an autoimmune basis that was missed because the relevant antibody tests weren't ordered. If you have idiopathic neuropathy with any features of immune involvement — relatively rapid onset, asymmetric symptoms, weakness in addition to sensory changes, family history of autoimmune disease, or other autoimmune symptoms — it's reasonable to ask for a more thorough autoimmune workup.
What conditions cause autoimmune neuropathy as a secondary feature?
Many. Sjögren's syndrome, lupus, rheumatoid arthritis, celiac disease, inflammatory bowel disease, sarcoidosis, type 1 diabetes, and several vasculitis syndromes can all cause peripheral neuropathy as part of their broader autoimmune picture. If you have one of these conditions and develop new nerve symptoms, treating the underlying disease often improves the neuropathy.
Should I get genetic testing if I have autoimmune neuropathy?
Genetic testing isn't routine for autoimmune neuropathy, but it's sometimes done to rule out hereditary conditions like Charcot-Marie-Tooth that can mimic acquired neuropathy. Some research is ongoing into genes that increase autoimmune susceptibility, but actionable genetic testing for autoimmune neuropathy specifically is not yet standard. If you have a strong family history of autoimmune disease, mention it to your neurologist.