
Low-Dose Naltrexone (LDN) for Neuropathy: What Patients Are Reporting
Every few months, someone writes to me about a medication their doctor prescribed off-label that actually made a difference. Over the past two years, one name keeps coming up more than any other: low-dose naltrexone, or LDN. “It didn't cure my neuropathy,” one reader told me, “but for the first time in three years, I can sleep through the night without burning feet waking me up.” Stories like hers are becoming increasingly common — and the science is starting to catch up.
LDN is one of the most interesting developments in chronic pain management — not because it's new, but because an old drug is being used in a completely new way. Here's what we know, what we don't, and what you should consider before asking your doctor about it.
What Is Low-Dose Naltrexone?
Naltrexone is an FDA-approved medication typically prescribed at 50 mg daily for opioid use disorder and alcohol dependence. At that dose, it works by blocking opioid receptors in the brain, reducing cravings and the rewarding effects of alcohol and opioids.
Low-dose naltrexone is something entirely different. At doses between 1.5 mg and 4.5 mg — roughly one-tenth of the standard dose — naltrexone appears to work through completely different mechanisms. Instead of simply blocking opioid receptors, LDN modulates the immune system and reduces neuroinflammation. It's this anti-inflammatory, immunomodulatory effect that has caught the attention of pain researchers and neuropathy patients alike.
It's important to understand that LDN for neuropathy is an off-label use. The FDA has not approved naltrexone at low doses for pain management. But off-label prescribing is common in medicine — gabapentin, one of the most prescribed neuropathy medications, was originally approved for epilepsy.
How LDN Works for Nerve Pain
The mechanism behind LDN's pain-relieving effects is genuinely fascinating, and it operates on multiple levels:
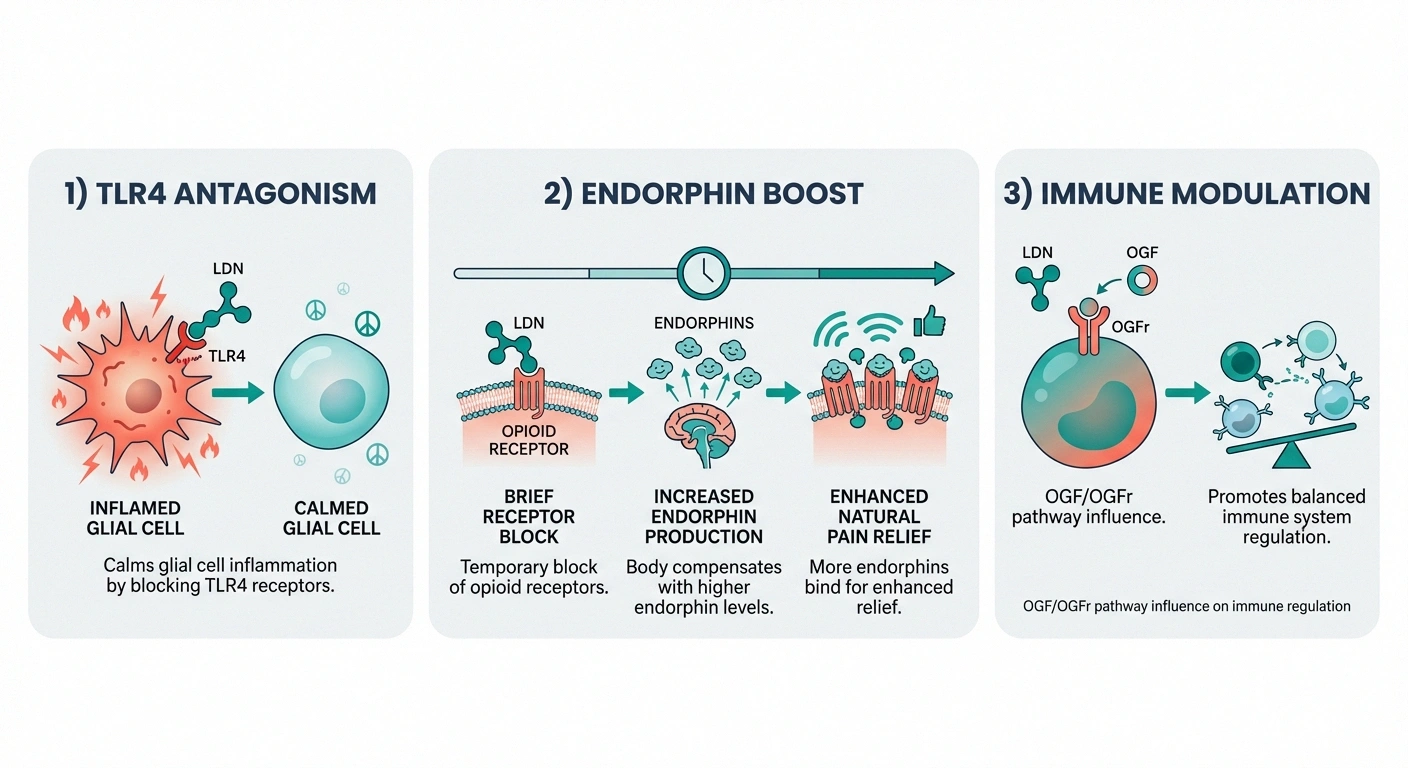

Reducing Glial Cell Inflammation
One of the most important discoveries about chronic neuropathic pain is the role of glial cells — immune-like cells in the nervous system. When nerves are damaged, glial cells become activated and release inflammatory mediators (cytokines like TNF-alpha, IL-6, and IL-1β) that amplify pain signals and create a feedback loop of chronic inflammation.
LDN works by blocking Toll-like receptor 4 (TLR4) on glial cells in both the central and peripheral nervous system. According to a comprehensive review published by the American Society of Regional Anesthesia (ASRA), this TLR4 antagonism reduces the glial inflammatory response and can reverse neuropathic pain. It's essentially calming down the overactive immune cells that are making your pain worse.
Boosting Endorphin Production
At low doses, naltrexone briefly blocks opioid receptors for only about 4 to 6 hours. During this brief blockade, your body responds by increasing production of endorphins — your natural painkillers — and upregulating opioid receptors. When the blockade wears off, you have more endorphins and more sensitive receptors to receive them. The net effect is enhanced natural pain relief. This is why LDN is typically taken at bedtime — the endorphin boost arrives by morning.
Modulating the Immune System
Through its effects on the Opioid Growth Factor (OGF) and Opioid Growth Factor Receptor (OGFr) pathway, LDN appears to influence immune cell proliferation and function. This broader immunomodulatory effect may explain why it has shown benefits across a range of autoimmune and inflammatory conditions — not just neuropathic pain.
What the Research Shows
Let me be straightforward about the evidence: it's promising but limited. We don't yet have the large, high-quality randomized controlled trials that would make LDN an established neuropathy treatment. But what does exist is genuinely encouraging.

Diabetic neuropathy: A randomized, double-blind crossover trial published in Journal of Diabetes Research tested LDN in patients with painful diabetic neuropathy. While the study was small, LDN showed efficacy in reducing pain with minimal side effects. The researchers noted it as a potentially safe alternative to conventional neuropathy drugs.
Small fiber neuropathy: A 2024 poster presented at the American Academy of Neurology annual meeting examined LDN in a cohort of patients with biopsy-confirmed cryptogenic small fiber neuropathy — the hardest-to-treat subtype. The results showed symptom improvement in a meaningful percentage of patients, though larger studies are needed to confirm these findings.
Neuropathic pain broadly: In a retrospective case series reviewed by the ASRA, patients with neuropathic pain conditions — including peripheral neuropathy and CRPS — showed more pronounced therapeutic response to LDN than patients with other pain types like arthritis. The authors described the effect as particularly evident in neuropathic conditions.
Fibromyalgia (related): The most robust LDN evidence comes from fibromyalgia research. A 2013 randomized controlled trial by Younger et al. found that 4.5 mg LDN produced significantly greater pain reduction than placebo in fibromyalgia patients. A 2017 pilot trial showed LDN decreased plasma levels of proinflammatory cytokines, providing objective evidence of its anti-inflammatory effect. Since fibromyalgia and neuropathy share mechanisms involving central sensitization, these findings have implications for neuropathy patients too.
Patient Reports: What People Are Actually Experiencing
Beyond the formal studies, the volume of patient reports about LDN for neuropathy is striking. Online communities like Mayo Clinic Connect are filled with detailed accounts:
- Pain reduction — Many patients report meaningful decreases in burning, shooting, and aching nerve pain. Not elimination — reduction. “Maybe 40-50% better” is a common description.
- Improved sleep — Reduced nighttime pain often translates to better sleep, which improves overall quality of life significantly.
- Fewer side effects than alternatives — Compared to gabapentin, pregabalin, or duloxetine, patients frequently report feeling clearer-headed on LDN.
- Gradual onset — Benefits typically don't appear immediately. Most patients report a 1 to 3 month delay before noticing improvement.
- Some non-responders — Not everyone benefits. Some people try LDN for several months with no noticeable change.
Patient reports are not clinical evidence, but the consistency of these experiences across thousands of people is notable. Combined with the mechanistic research, it paints a picture worth paying attention to.
How LDN Compares to Standard Neuropathy Medications
To put LDN in context, here's how it stacks up against the medications most commonly prescribed for neuropathic pain:
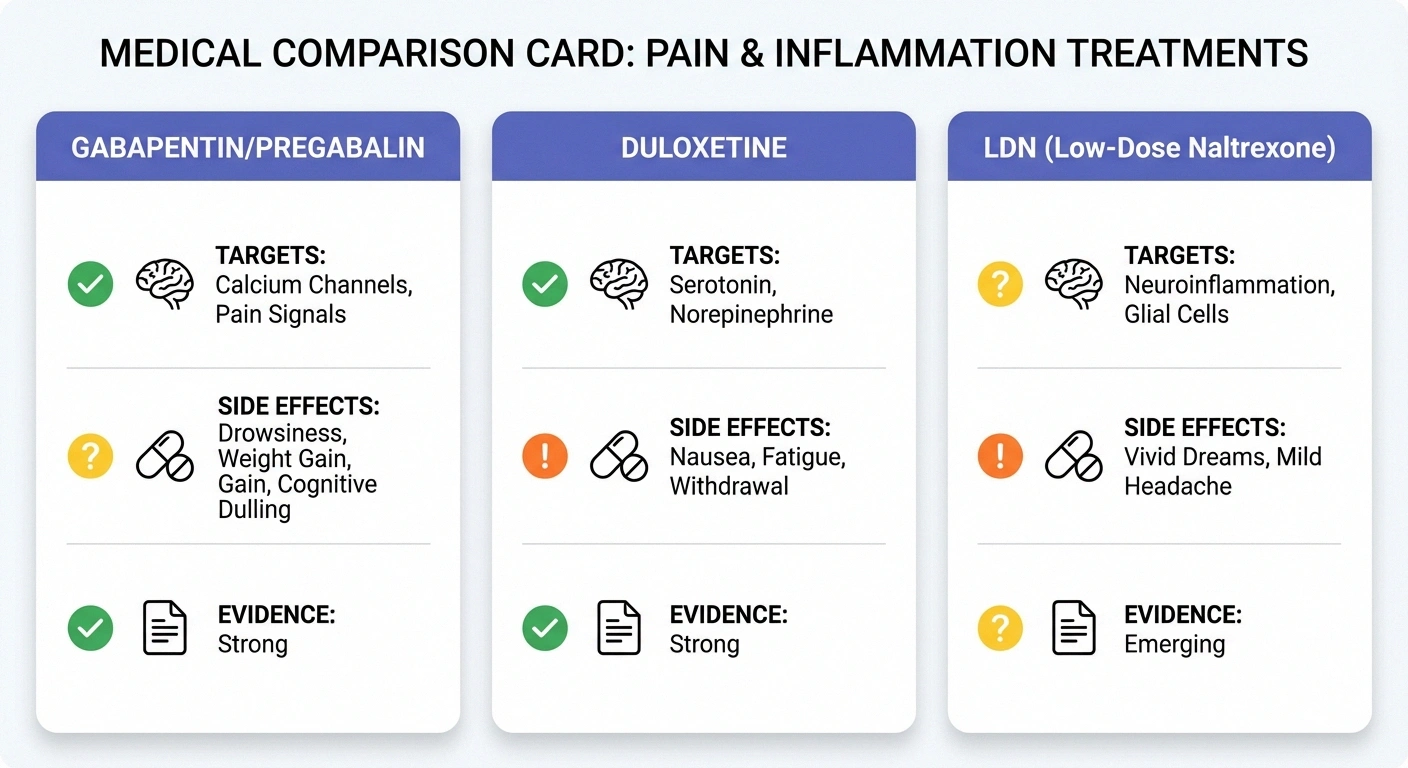
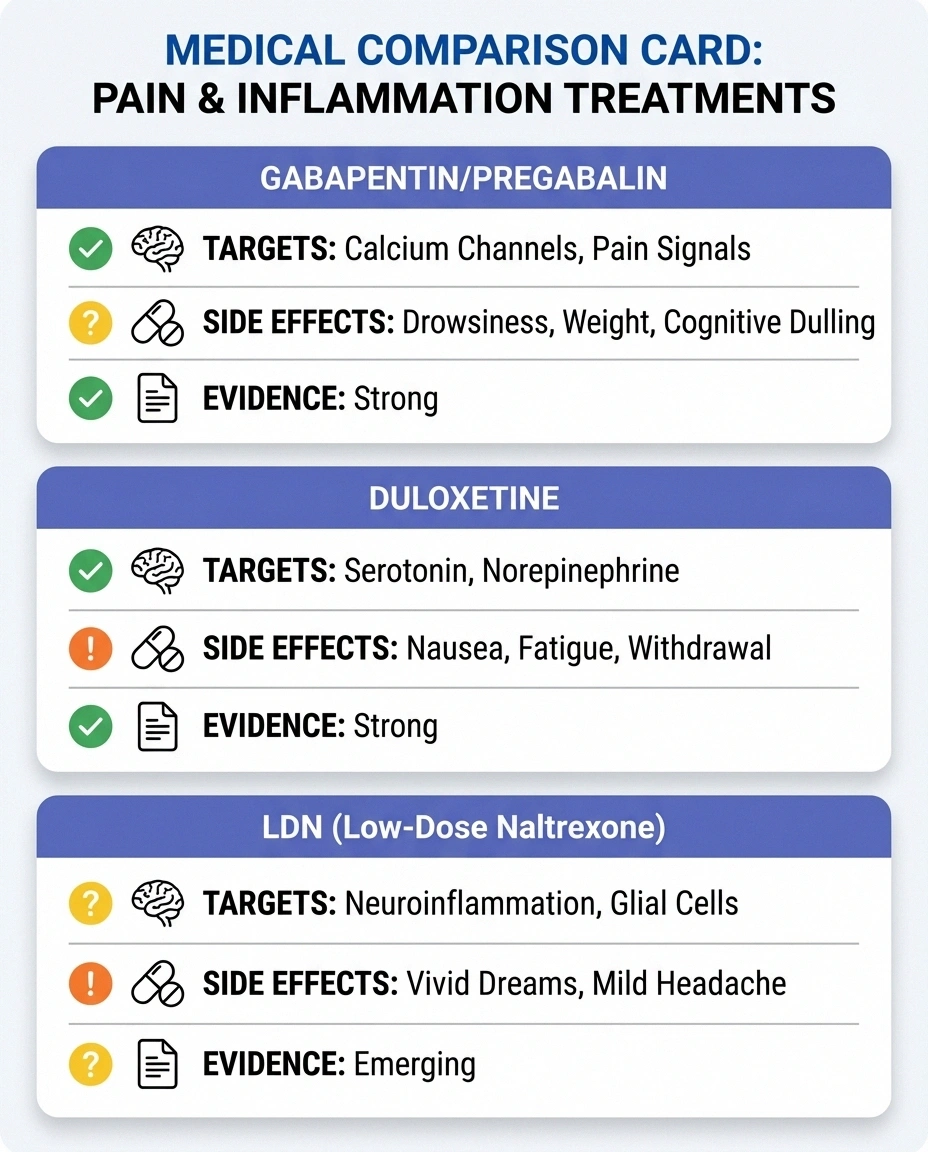
Gabapentin/Pregabalin: These are first-line treatments with extensive clinical evidence. They work well for many patients but carry side effects including drowsiness, cognitive dulling, dizziness, weight gain, and sometimes dependence. They treat symptoms only — they don't address underlying inflammation.
Duloxetine (Cymbalta): An SNRI antidepressant with FDA approval for diabetic neuropathy pain. Effective for many, but side effects include nausea, dry mouth, fatigue, and difficult withdrawal. Again, symptom management rather than mechanism-based treatment.
LDN: Targets neuroinflammation rather than just blocking pain signals. Side effect profile is generally milder — vivid dreams, mild headache, and occasional sleep disruption are the most commonly reported. Much less evidence supporting it, and it requires a compounding pharmacy. But its mechanism of action is fundamentally different — it's trying to reduce the inflammatory process rather than mask the pain.
Most LDN prescribers position it as an adjunct or alternative when standard medications have failed, caused intolerable side effects, or produced only partial relief. It's not a replacement for first-line treatments that have solid evidence — it's an option when those treatments fall short.
What to Know Before Asking Your Doctor
If LDN sounds like something worth exploring, here's what you need to know before the conversation:

Dosing and Titration
LDN is typically started at 1.5 mg at bedtime and slowly titrated up over 2 to 3 months to the target dose of 4.5 mg. This gradual approach minimizes side effects. Some practitioners start even lower at 0.5 mg. The target dose range for pain management is typically 1.5 to 4.5 mg daily, though some clinicians use doses up to 7 to 10 mg. Higher doses have not been shown to produce better results.
Compounding Pharmacies
Because naltrexone is only commercially available as a 50 mg tablet, LDN must be prepared by a compounding pharmacy at the correct low dose. This means it's only available by prescription and requires a doctor willing to prescribe it. Not all pharmacies compound LDN, so you may need to find one that specializes in it.
Insurance Coverage
Most insurance plans do not cover LDN since it's an off-label, compounded medication. Out-of-pocket costs vary but are generally modest — typically $30 to $60 per month, which is often less than copays for brand-name neuropathy medications. This relative affordability is one reason LDN has gained traction.
Drug Interactions
Critical: LDN cannot be taken with opioid medications. Because naltrexone blocks opioid receptors, taking it alongside opioids will block their pain-relieving effects and can precipitate withdrawal. If you're currently taking any opioid medication — including tramadol — you must discuss this with your doctor before starting LDN. You'll typically need to be opioid-free for 7 to 14 days before beginning.
LDN is generally compatible with gabapentin, pregabalin, duloxetine, and most other non-opioid pain medications. In fact, some research suggests ultra-low-dose naltrexone may enhance the pain-relieving effects of gabapentin and pregabalin in neuropathic pain models.
Perioperative Considerations
If you're scheduled for surgery, inform your surgical team that you're taking LDN. The Low Dose Naltrexone Research Trust recommends stopping LDN 2 days before surgery and restarting 2 days after you've stopped taking any post-operative opioids. Since LDN upregulates opioid receptors, opioid dosing during and after surgery may need careful adjustment.
Side Effects and Safety
One of LDN's most attractive features is its safety profile. In multiple studies and large retrospective reviews, serious adverse effects have been rare. The most commonly reported side effects include:
Availability: Compounding pharmacy only — requires a prescription
Typical timeline: Start at 1.5 mg, titrate to 4.5 mg over 2-3 months
When to take: Usually bedtime, though some switch to morning if vivid dreams are bothersome
Time to effect: 1-3 months at target dose before you'll know if it's working
- Vivid dreams — The most common complaint, occurring in the first few weeks. Often resolves on its own or with dose adjustment. Some patients switch from nighttime to morning dosing to manage this.
- Mild headache — Usually temporary and responds to dose reduction.
- Sleep disturbance — Some patients experience initial insomnia, which typically improves as the body adjusts.
- Nausea — Uncommon but occasionally reported, especially at higher doses.
A retrospective review of 215 multiple sclerosis patients on LDN described the medication as “safe with negligible adverse effects.” Multiple other studies have reached similar conclusions. This favorable safety profile, combined with its low cost, is what makes LDN worth discussing — even though the evidence base for neuropathy specifically is still developing.
Who May Benefit Most from LDN
Based on the available evidence and clinical experience, LDN may be worth exploring if you:

- Have neuropathic pain that hasn't responded well to gabapentin, pregabalin, or duloxetine
- Experience intolerable side effects from standard neuropathy medications
- Have small fiber neuropathy, which is notoriously difficult to treat with conventional drugs
- Have an autoimmune component to your neuropathy (lupus, Sjögren's, CIDP)
- Want to try an approach that targets inflammation rather than just masking symptoms
- Cannot take opioids or want to avoid them
At the University of Virginia Medical Center, their pain practice prescribes LDN for fibromyalgia and neuropathic pain conditions that are refractory to first- and second-line medications — positioning it as a last-resort option when other approaches have been exhausted.
Finding a Doctor Who Prescribes LDN
This can be one of the biggest hurdles. Because LDN is off-label and the evidence base is still developing, many physicians aren't familiar with it or are hesitant to prescribe it. Here are some practical steps:
- Start with your neurologist or pain specialist. Bring printed copies of the studies mentioned in this article. Frame it as: “I've read about this emerging option and want your professional opinion.”
- Ask about integrative medicine. Doctors in integrative or functional medicine practices are often more familiar with LDN.
- Check the LDN Research Trust (ldnresearchtrust.org) for provider directories and educational resources.
- Be patient with the process. If your doctor agrees to try LDN, expect a 1 to 3 month titration period before you'll know if it's working for you.
Frequently Asked Questions
How long does LDN take to work for neuropathy?
Most patients report noticing benefits between 1 and 3 months after reaching their target dose. Some clinicians recommend a 3-month trial at the full dose before concluding it isn't effective. Initial side effects like vivid dreams usually resolve within the first few weeks.
Can I take LDN with gabapentin?
Yes, LDN is generally compatible with gabapentin, pregabalin, and other non-opioid neuropathy medications. Some evidence suggests the combination may be more effective than either alone. Always confirm with your prescribing doctor.
Is LDN safe long-term?
Available evidence suggests LDN has a favorable long-term safety profile. Some patients have taken it for years without significant issues. However, long-term controlled studies are limited, so ongoing monitoring with your doctor is recommended.
Does LDN help with numbness or just pain?
Most patient reports focus on pain reduction rather than improvement in numbness or tingling. LDN appears more effective for the inflammatory pain component of neuropathy than for sensory loss. As one patient summarized: it got rid of the pain but did nothing for the numbness.
Will LDN cure my neuropathy?
LDN is not a cure for neuropathy. It may reduce pain and inflammation, improve quality of life, and work alongside other treatments — but it does not reverse existing nerve damage. Think of it as a management tool, not a cure. For information about nerve healing, visit our guide on nerve regeneration and healing.
The Bottom Line
Low-dose naltrexone represents something genuinely different in the neuropathy treatment landscape: a medication that targets the inflammatory process driving nerve pain rather than simply dampening pain signals. The evidence is still developing — we need larger, more rigorous trials — but what exists is encouraging, the safety profile is favorable, and the cost is low.
If you've tried the standard neuropathy medications and they haven't worked or have caused problems, LDN is worth discussing with your doctor. It may not work for everyone, and it requires patience — but for the patients who do respond, it can meaningfully improve quality of life with minimal downsides.
For more on managing neuropathic pain, explore our comprehensive guides to neuropathy medications and natural remedies for peripheral neuropathy. And if you're interested in other emerging treatments, check out our coverage of scrambler therapy and spinal cord stimulation for neuropathy.


