When the numbness or burning first showed up in my feet, the question that kept me awake wasn't “how do I treat this?” It was “why is this happening to me?” I'd never had a serious illness. I wasn't a heavy drinker. I didn't understand how a person just… develops nerve damage. It turned out there isn't one answer to that question — there are dozens, and they range from the very common to the genuinely rare, from the easily treatable to the lifelong.
This is the guide I went looking for back then and couldn't find in one place: a plain-language tour of essentially every known cause of peripheral neuropathy, organized so you can actually navigate it, with a path into a deeper article on each one. A word before we start: this is a map, not a diagnosis. Many of these causes look alike from the outside, and pinning down your specific cause is a job for your doctor, using your history, an exam, and tests — we walk through that process in our guide to how neuropathy is diagnosed. Use this to understand the landscape and to ask sharper questions, not to self-diagnose at midnight.
How Doctors Think About the Causes
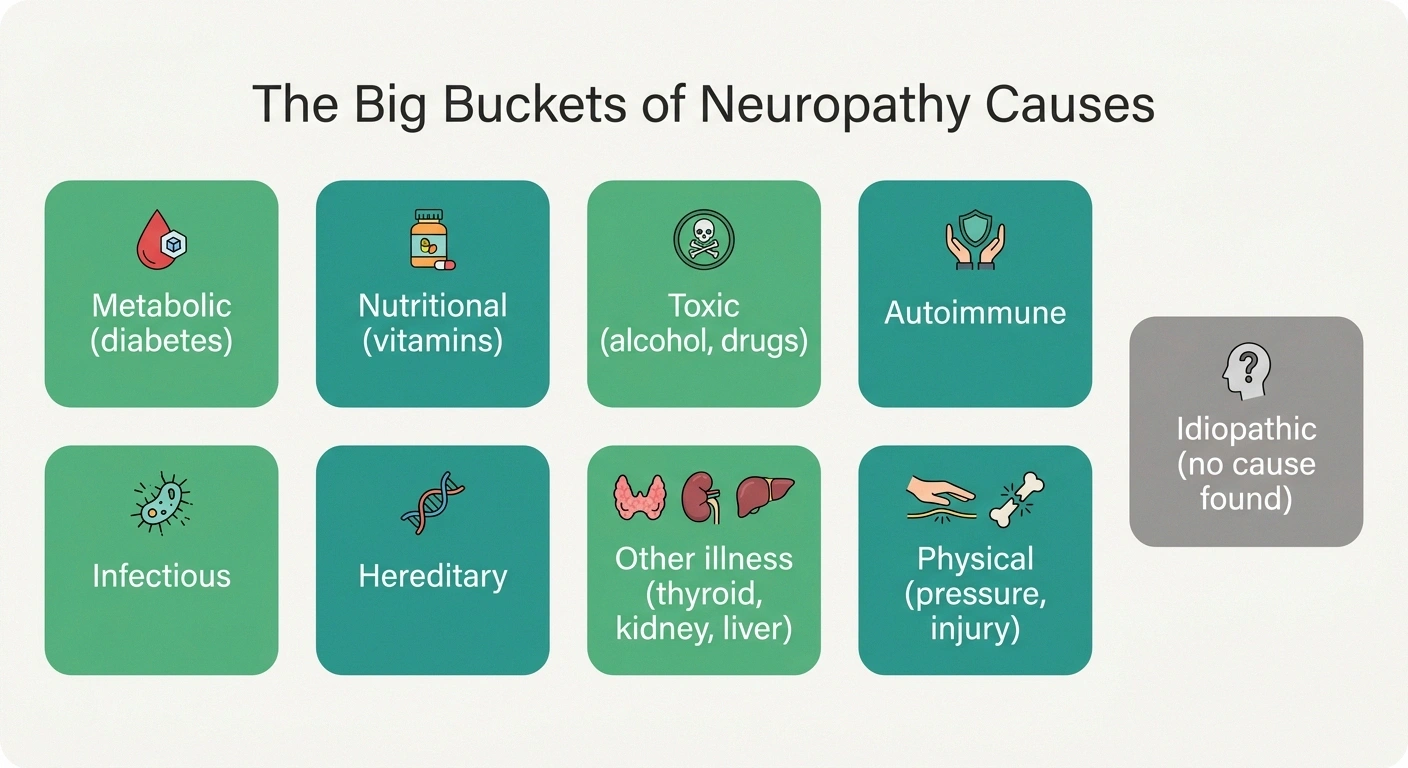
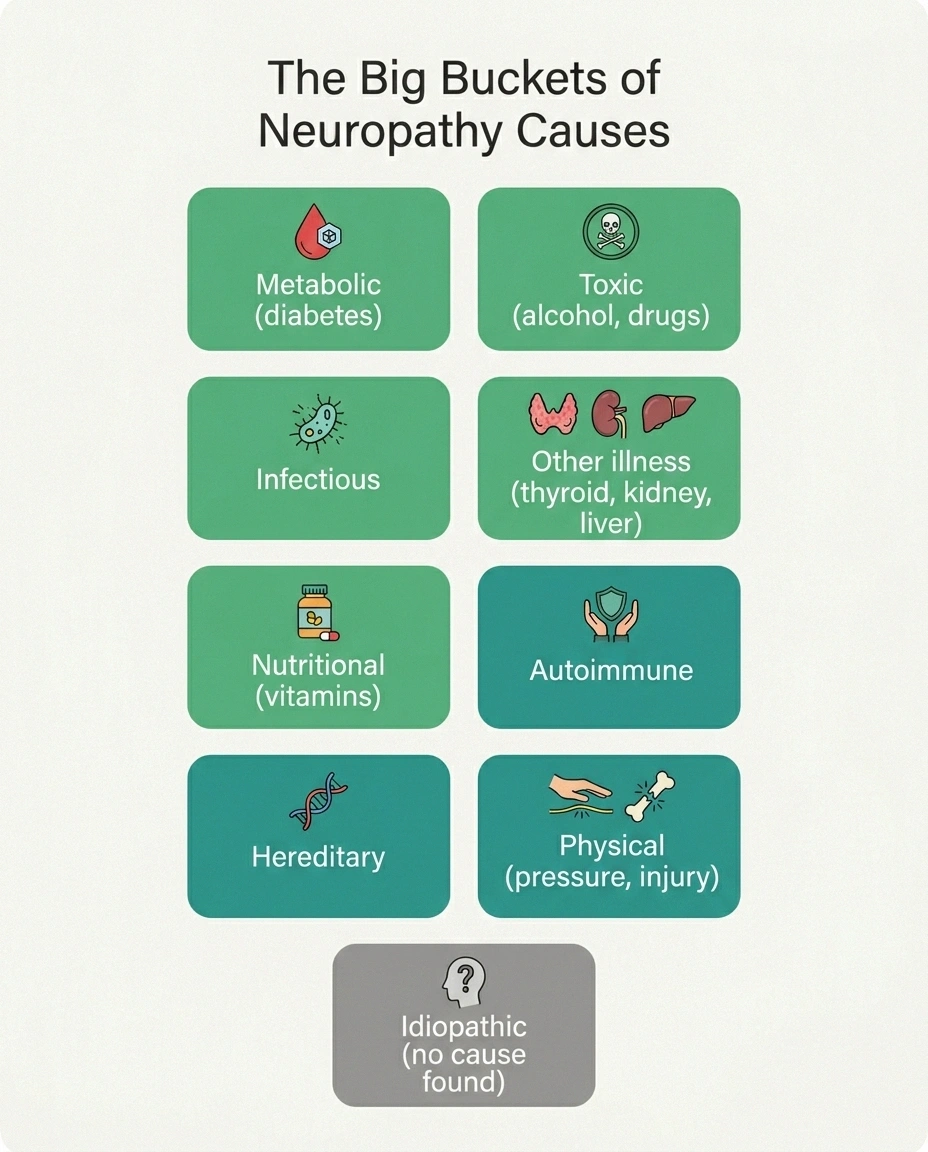
Doctors don't memorize a random list of a hundred causes. They sort them into a handful of big buckets and work through them: metabolic (like diabetes), nutritional (vitamin problems), toxic (alcohol, certain drugs, environmental poisons), autoimmune and inflammatory, infectious, hereditary, other systemic illnesses (thyroid, kidney, liver), and physical or mechanical causes like pressure and injury. And then there's a final, important category: idiopathic, which simply means no cause was found despite a thorough search.
A meaningful number of these causes are treatable
And a few are partly reversible if caught early. That is exactly why identifying the cause is the single highest-leverage thing you and your doctor can do — not bureaucratic thoroughness.
Holding those buckets in mind makes the rest of this article — and your own results — far less overwhelming. Here's the single most encouraging fact to carry through all of it: a meaningful number of these causes are treatable, and a few are partly reversible if they're caught early. That's why identifying the cause is the highest-leverage thing you and your doctor can do. We come back to that at the end.
Diabetes and Blood Sugar: The Biggest Single Cause

If there's one cause to know, it's this one. Diabetes is the most common cause of peripheral neuropathy in countries like ours; a large share of people with diabetes develop some degree of nerve damage over time. Persistently high blood sugar injures the small blood vessels that feed your nerves and damages the nerves directly. Our overview of diabetic neuropathy covers how it develops and what slows it down.
Nerve damage can begin in the prediabetic range, while standard tests still read borderline — a pattern many people and even some clinicians overlook. Because blood sugar is so common and so actionable, it is almost always investigated first.
Crucially, you don't have to have full diabetes for blood sugar to be the culprit. Nerve damage can begin in the prediabetic range, when standard tests still look borderline — a pattern many people and even some clinicians overlook, which we dig into in prediabetes and neuropathy. Because blood sugar is so common and so actionable, it's almost always investigated first.
Alcohol
Alcohol causes neuropathy by two routes at once: it's directly toxic to nerves, and heavier drinking tends to come with the poor nutrition (especially B-vitamin deficiency) that independently damages nerves. The result is a fairly recognizable pattern of burning, numb feet. The hopeful part is that this is one of the more modifiable causes — reducing or stopping alcohol, paired with nutritional repair, can halt the progression and sometimes allow partial recovery. Our article on alcoholic neuropathy handles this honestly and without judgment, because shame keeps people from getting help they could benefit from.
Vitamin Problems — Too Little, and Sometimes Too Much

Nutrition is a classic and very treatable cause, which is why it's worth understanding well. The most important deficiency is vitamin B12; low B12 produces a neuropathy that can improve with proper repletion, and the catch is that a “normal-looking” B12 level can still be functionally low — our guides to vitamin deficiencies that cause neuropathy and to B12 injections versus oral supplements explain the nuance. Deficiencies of vitamin B1 (thiamine), vitamin E, and copper can do the same.
The Cause Hiding in the Supplement Drawer
With vitamin B6, too much is also a cause. High-dose B6 — often taken without realizing the dose has stacked across several products — can itself produce a sensory neuropathy. “Natural” and “more” are not the same as “safe.” Auditing your own supplements is a specific, worthwhile step.
Here's the part almost nobody expects: with vitamin B6, too much is also a cause. High-dose B6 supplementation, often taken without anyone realizing the dose has crept up across multiple products, can itself produce a sensory neuropathy. It's a humbling reminder that “natural” and “more” are not the same as “safe,” and it's a specific thing worth auditing in your own supplement drawer.
Chemotherapy and Other Medications

A number of medications can damage peripheral nerves, and the most significant is chemotherapy. Several chemo drug families commonly cause chemotherapy-induced peripheral neuropathy (CIPN), which can begin during treatment and sometimes lingers afterward; it's important enough that we cover it in depth in chemo-induced neuropathy. Beyond chemo, a range of other drugs are recognized contributors — certain antibiotics, some heart-rhythm and seizure medications, and others — which we catalog in medications that can cause neuropathy. Cholesterol-lowering statins are a frequently asked-about and less common contributor, addressed specifically in statin-induced neuropathy.
The practical takeaway isn't to fear your medications — most people take these drugs without nerve problems, and stopping a needed medication on your own can be dangerous. It's to make sure every prescriber and your pharmacist have your full list, so a drug-related contribution can be spotted and weighed deliberately rather than missed.
Autoimmune and Inflammatory Diseases
Sometimes the immune system, which is supposed to defend the body, attacks the nerves instead. This category matters because several of its members are treatable, sometimes urgently so. Guillain-Barré syndrome is the acute, rapidly progressing form and is a medical emergency — we describe its warning pattern in Guillain-Barré syndrome. Its chronic cousin, CIDP, develops and persists more slowly and is specifically treatable; see CIDP explained.
Rapidly progressing weakness is a medical emergency
Most causes here are slow. Guillain-Barré syndrome is the exception — fast-spreading weakness and numbness, often rising from the feet upward over days, needs urgent medical care, not a wait-and-see. When in doubt, seek help promptly.
Systemic autoimmune diseases can also involve the nerves: lupus (lupus and neuropathy), the various forms of vasculitic neuropathy, rheumatoid arthritis, Sjögren's syndrome, sarcoidosis, and — more often than people expect — celiac disease, where gluten-related immune activity can show up as nerve symptoms even without dramatic digestive complaints. The reason your workup may include autoimmune blood tests is precisely that this bucket hides treatable causes.
Infections

Several infections can damage nerves, either directly or by triggering an immune response. The well-recognized ones include HIV, hepatitis C — covered in hepatitis C and neuropathy — Lyme disease, and syphilis. Shingles deserves a special mention: after the rash resolves, it can leave behind a persistent, often severe nerve pain in the affected area, which we address in post-herpetic neuralgia. And more recently, a number of people have reported new nerve symptoms following viral illness, including COVID — see neuropathy after COVID. These are on standard workup checklists for a good reason: treating the underlying infection can change the course of the neuropathy.
Inherited (Genetic) Neuropathies
Some neuropathies are written into the genes. The most common inherited group is Charcot-Marie-Tooth disease, a family of conditions that typically begin earlier in life and often run in families, with patterns like high arches, foot deformity, and difficulty with balance and gait — our article on hereditary neuropathy and Charcot-Marie-Tooth goes through it. There are also hereditary forms of amyloid neuropathy, some of which now have specific treatments — a genuinely hopeful development in a category that was historically frustrating. A family history of unexplained nerve problems, foot deformities, or “everyone in our family has bad feet” is the kind of clue worth mentioning to your doctor, because it can redirect the whole investigation.
Other Medical Conditions: Thyroid, Kidney, and Liver

Several whole-body illnesses can quietly damage nerves as a side effect of their disruption to your metabolism. An underactive thyroid is a classic and very treatable example — see thyroid problems and neuropathy. Chronic kidney disease can produce a neuropathy related to the buildup of substances the kidneys would normally clear, and chronic liver disease can do something similar. There are also neuropathies linked to abnormal proteins (monoclonal gammopathy and amyloidosis) and, less commonly, to cancer through paraneoplastic syndromes, where the nerve problem can even precede the cancer's discovery. This is why a neuropathy workup includes a broad metabolic panel — it's checking these systems, not padding the bill.
Toxins and Environmental Exposures
Beyond alcohol and medications, certain toxins damage nerves: heavy metals such as lead, arsenic, mercury, and thallium, along with some industrial solvents and pesticides. Our guide to toxic neuropathy covers this category and, importantly, its outlook. One nuance worth knowing — because it cuts against the instinct to “test for everything” — is that broad heavy-metal testing is generally only useful when there's a real exposure history (an occupation, a hobby, a known source). Without that, a “positive” is far more likely to be a false alarm than a true finding. So this is a cause that's pursued by history first, not by reflexively ordering every panel.
Physical Causes: Pressure, Trauma, and Surgery
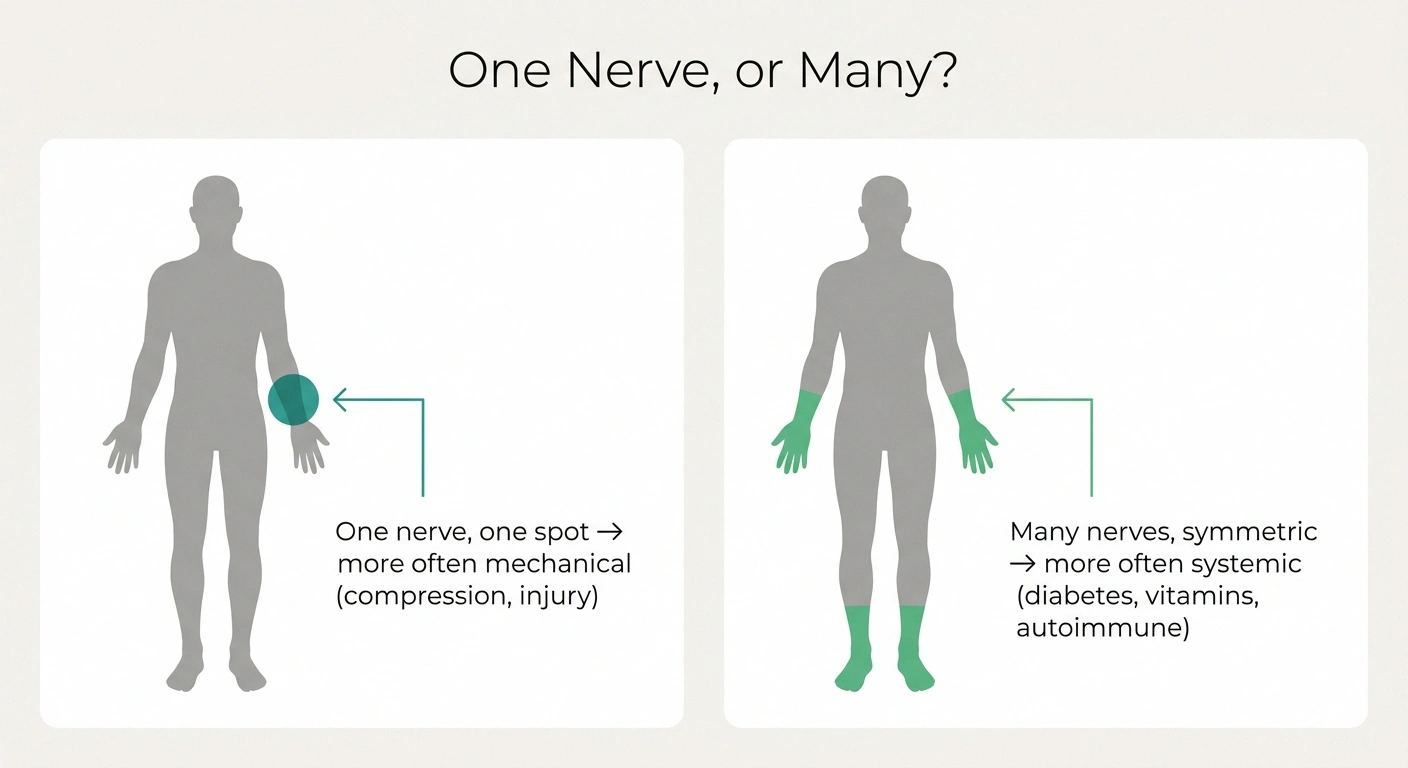
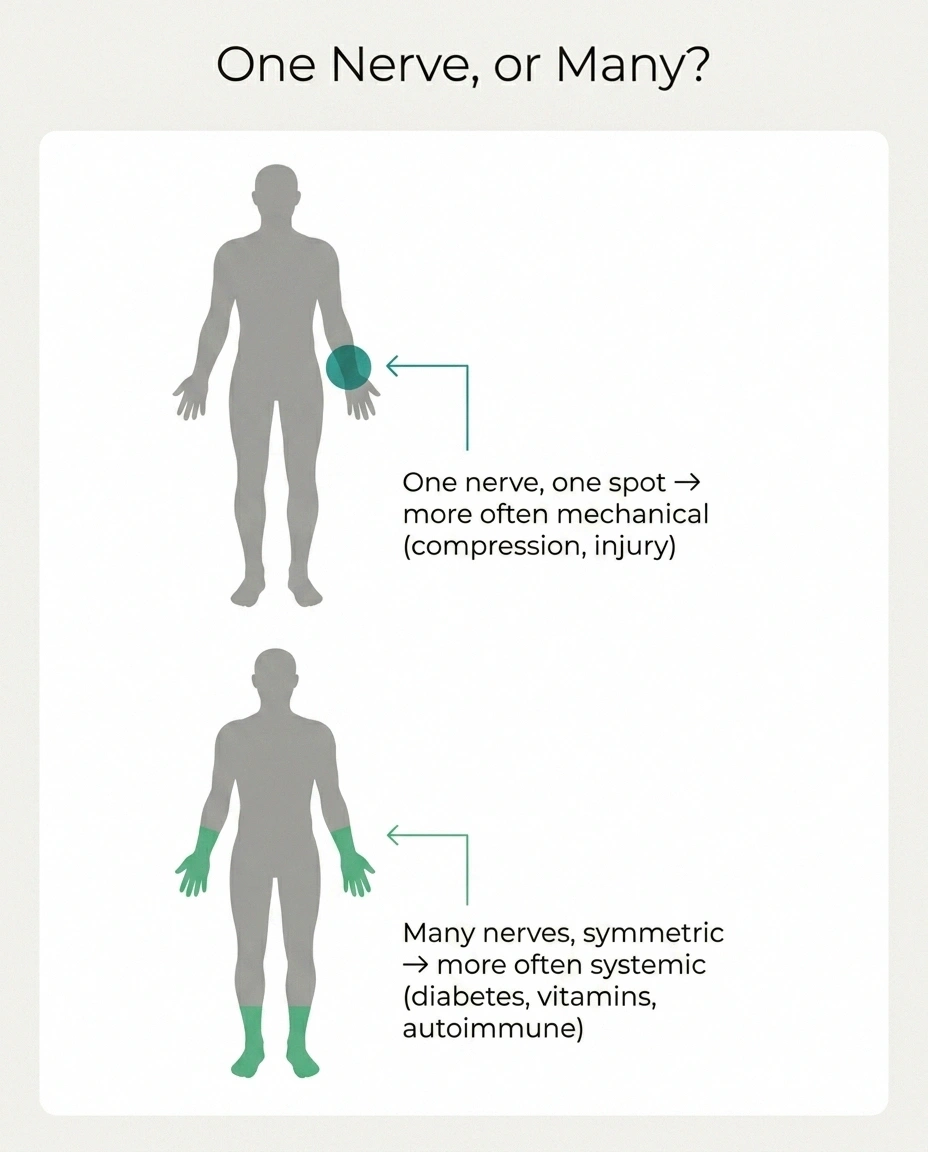
Not every neuropathy is metabolic or systemic. Sometimes a nerve is simply being compressed, stretched, or injured. Entrapment problems like carpal tunnel syndrome are the everyday example — a single nerve squeezed at a vulnerable spot. Trauma, fractures, and repetitive stress can injure nerves directly, and nerve symptoms sometimes appear after an operation, which we discuss in neuropathy after surgery. A useful distinction lives here: when one nerve in one location is affected, the cause is more likely mechanical; when many nerves are affected symmetrically (the classic “stocking-glove” pattern in both feet, then hands), a systemic cause like the ones above is more likely. That pattern is one of the first things a clinician reads, and it's part of why the location and symmetry of your symptoms matter so much.
When the Cause Is “Unknown”: Idiopathic Neuropathy

Here's a fact that surprises and, frankly, upsets a lot of people: even after a careful, thorough workup, a sizable share of neuropathy — often roughly a quarter to a third of cases — has no identifiable cause. This is called idiopathic neuropathy, and it becomes more common with age. I want to be careful and honest about what this means, because it's so easy to mis-hear.
What “Idiopathic” Does and Doesn't Mean
Imaginary. Untreatable. The end of the road. A statement that nothing can be done for your symptoms.
The search didn't surface a named driver this time. Symptom care still applies, lifestyle still matters, and a cause sometimes declares itself later — so follow-up over time is worthwhile.
Idiopathic does not mean “imaginary,” and it does not mean “untreatable.” It means the search didn't surface a specific, named driver this time. Symptom management still applies, lifestyle factors still matter, and sometimes a cause declares itself later and is worth re-checking for over time. Our article on idiopathic neuropathy is written specifically for the person who has been told “we couldn't find a reason” and is trying to figure out what that actually means for them. It is a recognized medical category, not a verdict that nothing can be done.
A Note on Patterns: Why the Same Symptoms Have Many Causes

One thing that confuses people is that wildly different causes can produce surprisingly similar symptoms — burning, numb feet can come from diabetes, B12 deficiency, alcohol, chemotherapy, or no found cause at all. That's not a flaw in medicine; it's the nature of nerves, which have a limited vocabulary for distress. It's also why you can't reason backward from symptoms alone to a cause, and why two people with identical-sounding feet can need completely different treatment. The way clinicians cut through this is by reading the pattern — how fast it came on, which nerves and which fibers are involved, whether it's symmetric, what your history and tests show. If you want to understand how neuropathy tends to develop and progress over time regardless of cause, our guide to the stages of neuropathy is a good companion to this one. And the related question patients ask most — whether the damage can be undone — is handled honestly in can neuropathy be reversed.
Burning, numb feet can come from diabetes, B12 deficiency, alcohol, chemotherapy, or no found cause at all. Nerves have a limited vocabulary for distress. Clinicians cut through this by reading the pattern — onset speed, which fibers, symmetry, history — not the symptom alone.
Why Finding the Cause Matters So Much

If you take one idea away from this long tour, make it this. The reason your doctor digs for a cause isn't bureaucratic thoroughness — it's that the cause often determines what can actually be done. A B12 deficiency can be repleted. A thyroid problem can be treated. Blood sugar caught in the prediabetic window can be acted on before more damage accrues. An autoimmune neuropathy like CIDP has specific treatments. An offending medication can sometimes be changed. Even when a cause turns out to be one of the harder ones, naming it almost always sharpens the plan and removes the corrosive uncertainty of not knowing.
You have the map — partner on the search
Bring your full medication and supplement list, family history, exposures, and a clear account of how symptoms started and spread. The map was never meant to make you the navigator alone — it's so you can recognize the territory while someone qualified guides you through it.
So if you're at the start of this — symptoms, no answers yet — the most useful thing you can do is partner with your doctor on the search rather than wait passively for it. Bring your full medication and supplement list, your family history, any exposures, and a clear account of how your symptoms started and spread. You now have the map. The point of a map was never to make you the navigator alone — it's so you can recognize the territory while someone qualified helps you find your specific way through it.
Frequently Asked Questions
What is the most common cause of peripheral neuropathy?
Diabetes is the most common single cause in countries like the United States, and a large share of people with diabetes develop some degree of nerve damage over time. Importantly, blood sugar problems can begin causing nerve damage in the prediabetic range, before full diabetes is diagnosed, which is why blood sugar is almost always investigated first in a neuropathy workup.
What causes neuropathy besides diabetes?
Many things: alcohol, vitamin problems (especially B12 deficiency, and also B6 excess), chemotherapy and certain other medications, autoimmune and inflammatory diseases such as Guillain-Barré, CIDP, lupus, vasculitis and celiac disease, infections including HIV, hepatitis C, Lyme and shingles, inherited conditions like Charcot-Marie-Tooth, other illnesses such as thyroid, kidney and liver disease, toxins and heavy metals, and physical causes like compression, trauma, and surgery. A meaningful share remains idiopathic, meaning no cause is found.
Can neuropathy have no cause at all?
Effectively, yes, in the sense that after a thorough workup roughly a quarter to a third of cases have no identifiable cause and are called idiopathic. This is more common with increasing age. Idiopathic does not mean the symptoms are imaginary or that nothing can help; it means a specific driver was not found, symptom management still applies, and a cause sometimes becomes apparent later with follow-up.
Which causes of neuropathy are reversible or treatable?
Several are treatable and some are partly reversible if caught early, including vitamin B12 deficiency, thyroid dysfunction, blood sugar problems addressed in the prediabetic window, certain autoimmune neuropathies such as CIDP, alcohol-related neuropathy with reduced drinking and nutritional repair, and medication-related neuropathy when an offending drug can be safely changed. This is exactly why identifying the cause is the highest-priority step, and why a normal first workup is sometimes worth repeating over time.
Can more than one cause contribute at the same time?
Yes, and this is common. For example, a person may have both diabetes and a B12 deficiency, or alcohol-related nerve damage compounded by poor nutrition. Multiple contributors can stack, which is one reason a careful workup looks across categories rather than stopping at the first finding, and why treatment sometimes addresses several factors at once.
How does the doctor figure out which cause is mine?
By combining your history, a neurological exam, and targeted tests. The pattern matters a great deal: how quickly symptoms started, whether one nerve or many are involved, whether it is symmetric, and your medication, family, and exposure history. Blood tests then hunt for treatable causes, and nerve testing characterizes the damage. No single piece is interpreted in isolation; the diagnosis comes from putting them together, which is a job for your clinician rather than symptom-matching on your own.
Is neuropathy from a single pinched nerve the same as the systemic kinds?
Not quite. When one nerve in one location is affected, the cause is more often mechanical, such as compression or injury, and the approach is different. When many nerves are affected symmetrically, often starting in both feet, a systemic cause such as diabetes, a vitamin problem, or an autoimmune condition is more likely. The location and symmetry of symptoms are among the first clues a clinician uses to steer the investigation.