
Neuropathy and Diabetic Foot Ulcers: Prevention and Care
It often starts with something small — a blister from a new pair of shoes, a pebble in your sock, a tiny cut from trimming your toenails. For most people, these minor injuries heal without a second thought. But when neuropathy has stolen the feeling in your feet, you may not notice the damage until it's become something much more serious: a diabetic foot ulcer. As someone who has heard from hundreds of readers navigating this exact reality, I want to give you the practical, honest guide I wish every person with diabetic neuropathy received at diagnosis.
Why Neuropathy Makes Your Feet Vulnerable
To understand diabetic foot ulcers, you first need to understand why diabetic neuropathy turns ordinary feet into a high-risk situation. The connection between nerve damage and ulcers isn't random — it's a predictable chain of events that you can interrupt at multiple points.
Peripheral neuropathy in the feet causes three types of damage that work together to create the perfect conditions for ulcers:
Sensory neuropathy removes your built-in warning system. Your feet can no longer tell you about a sharp object in your shoe, a too-tight sock, or a developing hot spot. Pain is your body's alarm system — without it, injuries go unnoticed for hours or days.
Motor neuropathy weakens the small muscles in your feet, changing their shape over time. Toes may curl (hammertoes) or the foot arch may shift, creating new pressure points that your shoes weren't designed to accommodate. These pressure points become the sites where ulcers most commonly develop.
Autonomic neuropathy reduces sweating in your feet, leaving the skin dry, cracked, and vulnerable to breakdown. When skin loses its moisture barrier, even minor friction can create an opening for bacteria.
Add compromised blood circulation — common in diabetes — and you have wounds that form easily, go undetected, and heal slowly. According to a 2025 comprehensive review in the World Journal of Diabetes, approximately 15% of people with diabetes will develop a foot ulcer during their lifetime, and 14-24% of those with ulcers will ultimately require amputation.
How Foot Ulcers Form
Understanding the ulcer formation process helps you see exactly where prevention efforts matter most. The typical pathway from healthy foot to ulcer follows a predictable sequence.
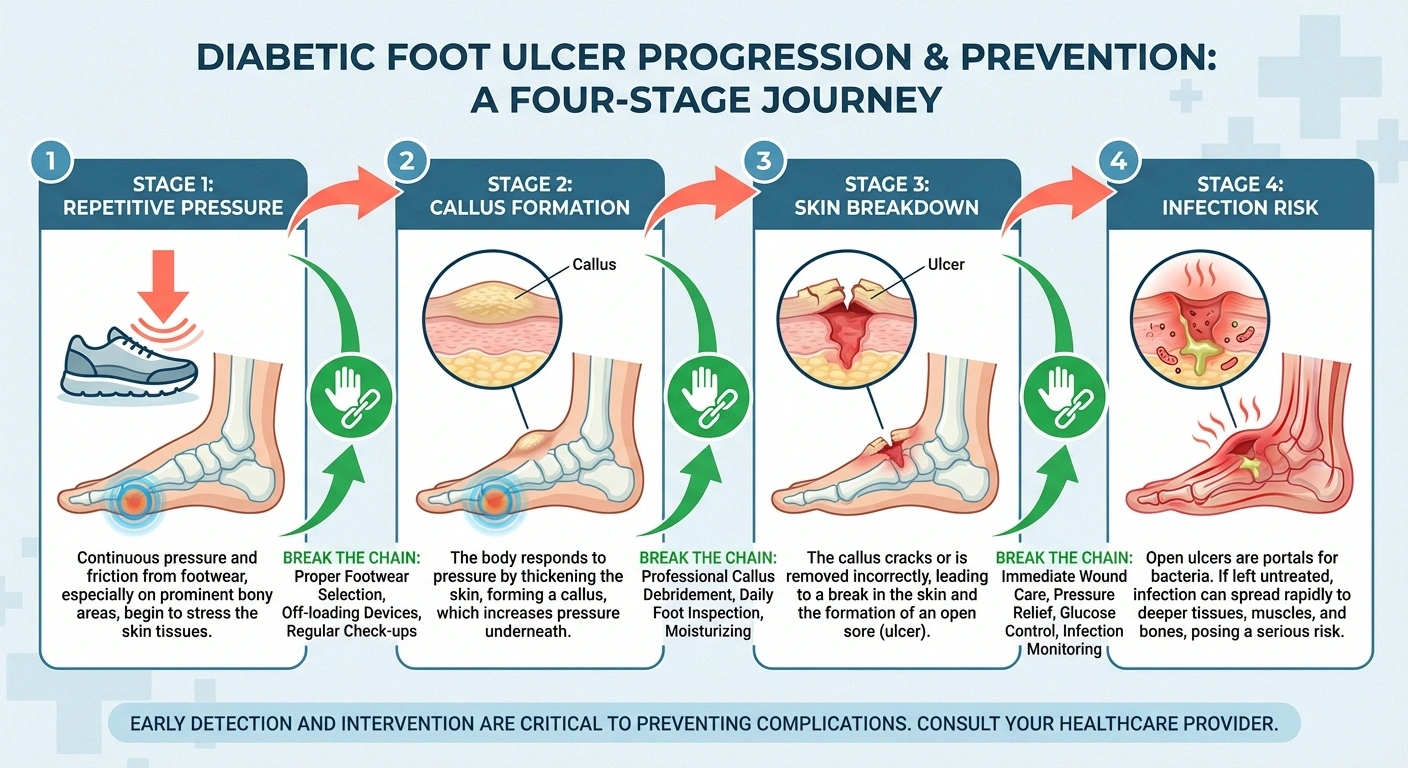
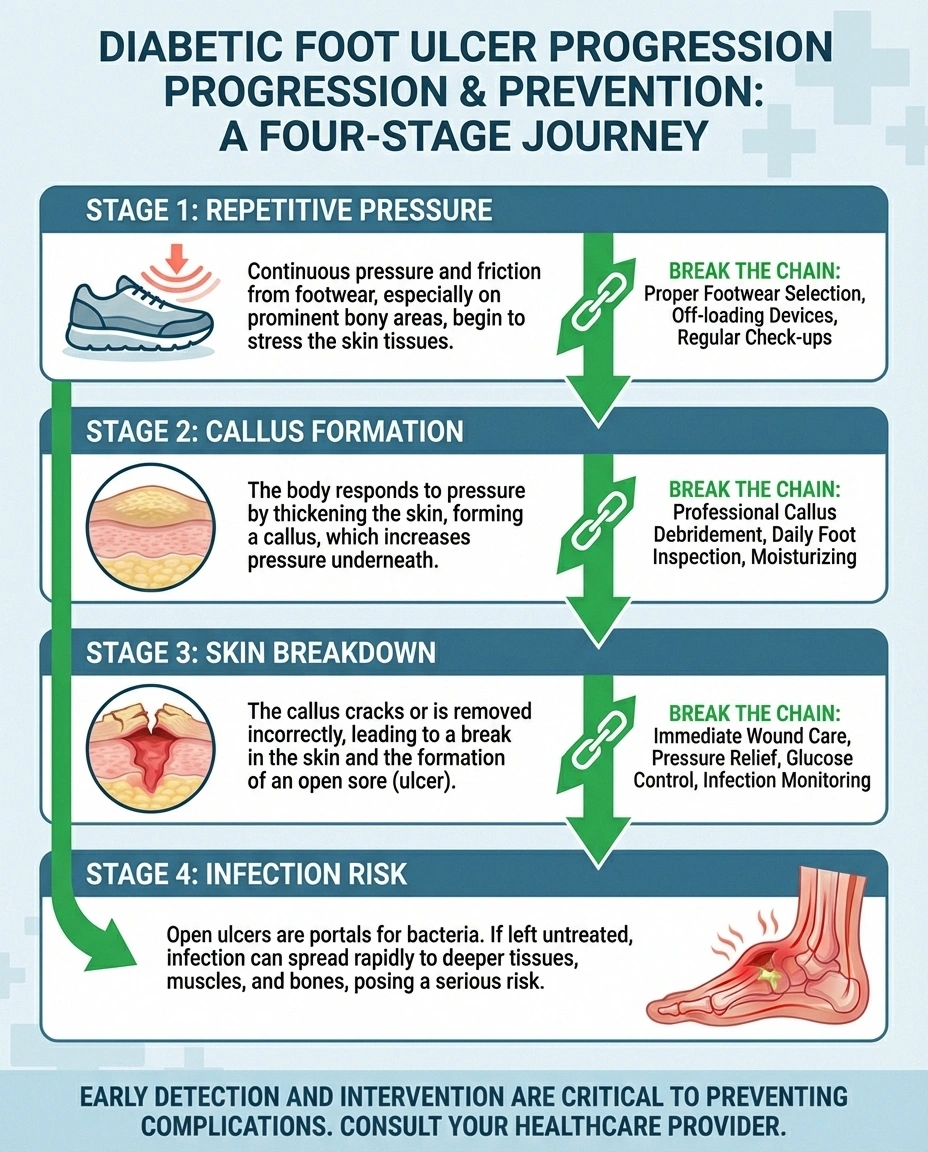
Stage 1: Repetitive pressure or friction. A specific spot on your foot experiences repeated stress — from a shoe seam, an area of bone prominence, or altered gait mechanics. In a foot with normal sensation, this pressure would cause discomfort, prompting you to adjust. With neuropathy, there's no signal to adapt.
Stage 2: Callus formation. The body responds to repetitive pressure by building up a callus — thickened skin designed to protect the area. While a callus seems protective, it actually increases pressure on the tissue beneath it. Research shows that calluses are a significant risk factor for ulcer development.
Stage 3: Skin breakdown. Continued pressure beneath the callus damages the tissue underneath. Eventually, the skin breaks down, creating an open wound. Because you can't feel this happening, the wound may already be quite deep before you notice it — perhaps only when you see blood on your sock or drainage in your shoe.
Stage 4: Infection risk. An open wound on a neuropathic foot with compromised blood flow becomes an invitation for bacterial infection. Infection in a diabetic foot can escalate rapidly from a surface issue to a deep tissue infection or bone infection (osteomyelitis) that threatens the limb.
Recognizing the Warning Signs
Since neuropathy means you may not feel a developing ulcer, you need to rely on visual checks instead. Here's what to watch for during your daily foot inspections:
- Color changes — Red, white, or dark discoloration on the bottom of your feet, between toes, or over bony areas
- Swelling — Unusual puffiness in one foot but not the other, or localized swelling over a joint or bone
- Temperature differences — One area feeling warmer or cooler than the surrounding skin (a sign of infection or reduced blood flow)
- Drainage — Any fluid on your socks, bandages, or inside your shoes
- Odor — An unusual or foul smell from your feet, which may indicate infection
- Callus changes — Bleeding within or beneath a callus, or a soft, mushy feeling when pressing on a callus
- Skin breakdown — Any open area, crack, blister, or cut that isn't healing normally
If you notice any of these signs, contact your healthcare provider promptly — don't wait for your next scheduled appointment. Early intervention is the single most important factor in preventing a small wound from becoming a limb-threatening ulcer.
The Classification System Your Doctor Uses
Doctors classify diabetic foot ulcers using the Wagner grading system, which measures severity from Grade 0 (intact skin with risk factors) to Grade 5 (gangrene of the entire foot). Understanding this classification helps you communicate with your medical team and grasp the seriousness of your situation.
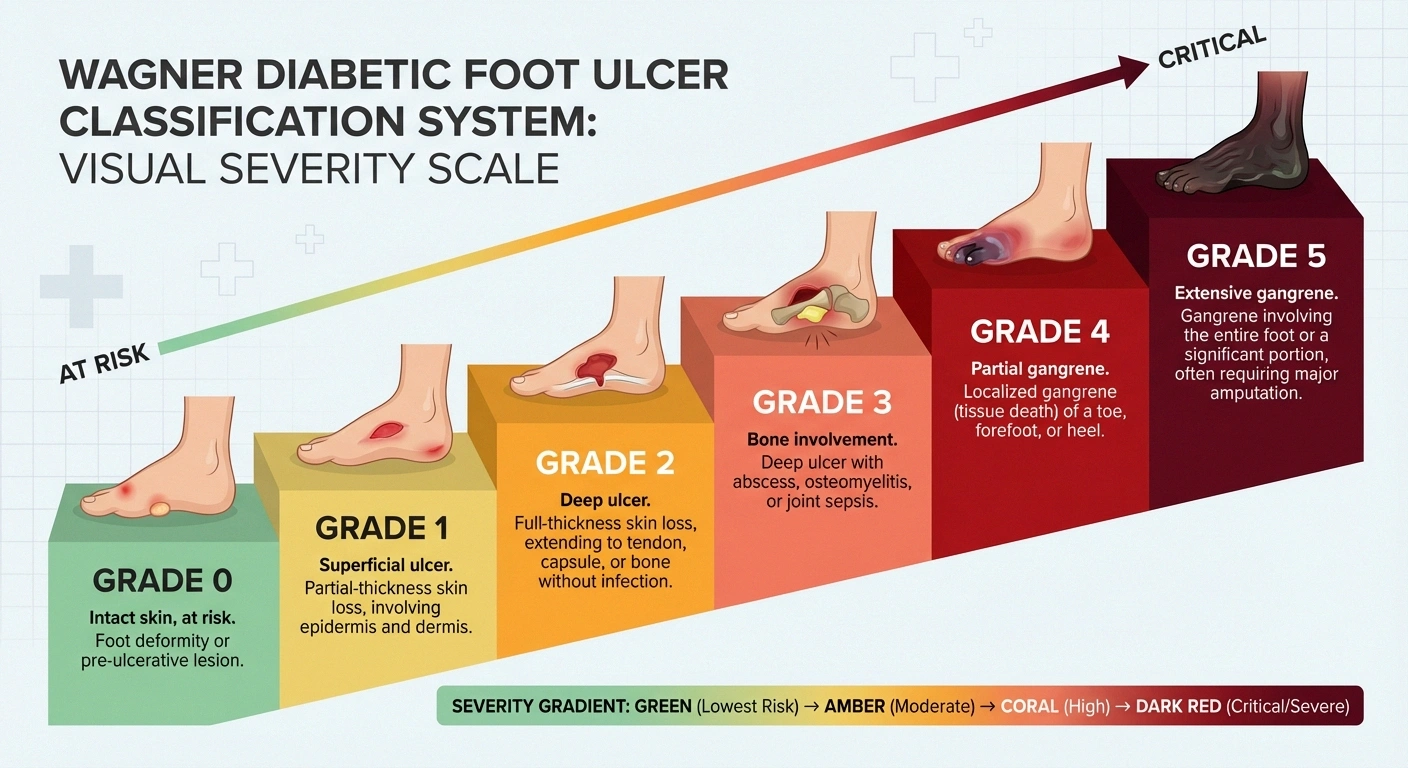
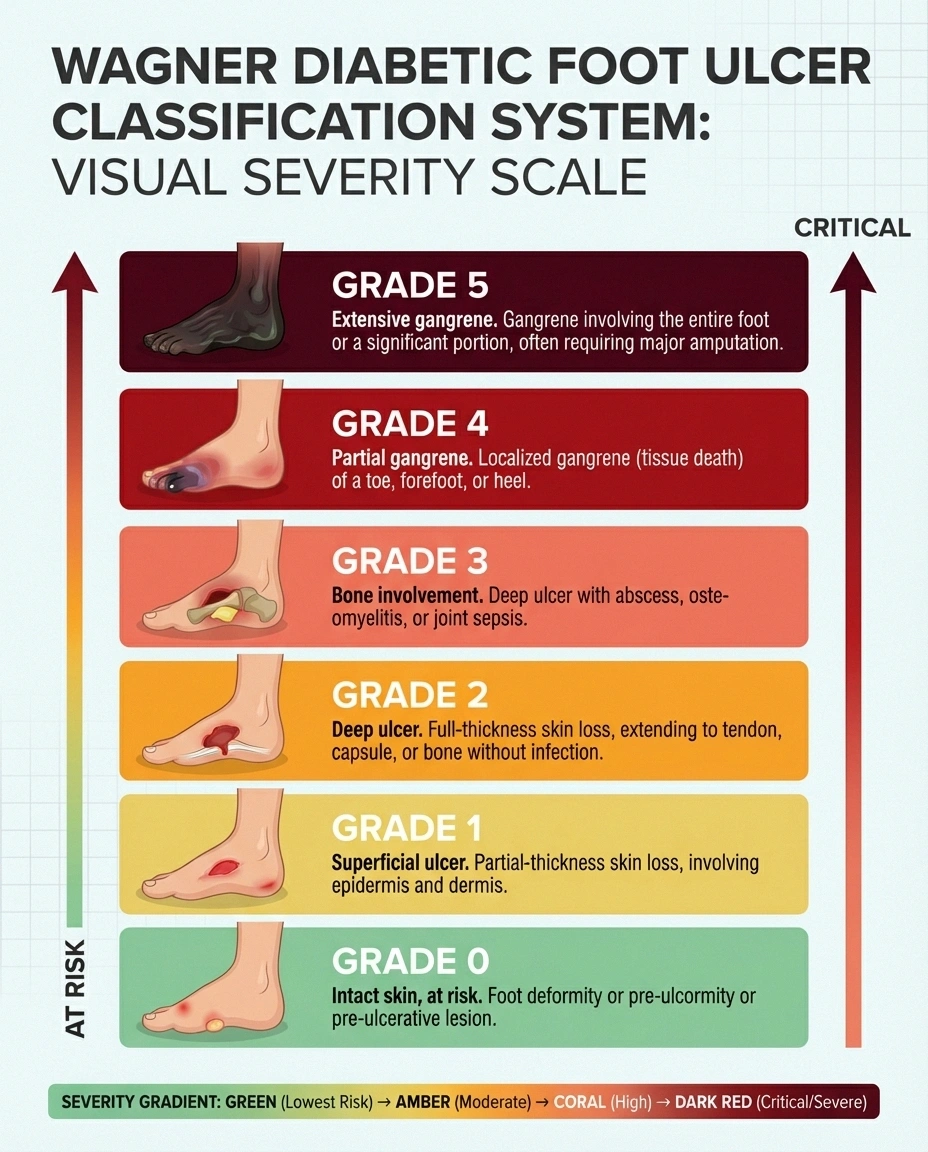
Grade 0: Skin is intact, but the foot is at risk due to neuropathy, deformity, or callus formation. This is the prevention stage — most of this article focuses on staying at Grade 0.
Grade 1: A superficial ulcer — the skin is broken but the wound is shallow, only involving the upper layers of skin.
Grade 2: A deep ulcer that extends through the skin into tendons, ligaments, or joint capsule, but no bone involvement yet.
Grade 3: A deep ulcer with bone visible or osteomyelitis (bone infection), or deep abscess formation.
Grades 4-5: Gangrene involving part of the foot (Grade 4) or the entire foot (Grade 5). These stages require urgent surgical intervention.
The goal of every prevention strategy in this article is to keep you at Grade 0 — intact skin, managed risk factors, and no open wounds.
Daily Foot Inspection: Your Most Important Habit
If you take away one thing from this article, let it be this: check your feet every single day. When neuropathy has removed your ability to feel problems, your eyes become your primary defense system.
What to check: Look at every surface of both feet — tops, bottoms, sides, between all toes, and around the nails. You're looking for cuts, blisters, redness, swelling, calluses, cracks, color changes, or anything that wasn't there yesterday.
How to check: If you can't easily see the bottoms of your feet, use a mirror placed on the floor, or ask a family member to help. Good lighting is essential — don't do a quick glance in dim light. Some people find it helpful to use a magnifying glass for a closer look, especially between the toes.
When to check: Build foot inspection into an existing daily routine so you never forget. Many people check their feet right before bed, after removing shoes and socks for the last time. Others prefer to check when getting out of the shower, when feet are clean and well-lit.
What to do if you find something: For minor findings like a small blister or superficial scrape, clean the area gently, apply antibiotic ointment, and cover with a clean bandage. Monitor it daily. If it isn't improving within 24-48 hours, or if you see signs of infection (increasing redness, warmth, swelling, discharge, or red streaks spreading from the wound), contact your healthcare provider immediately.
Footwear: Your First Line of Defense
The right shoes can prevent the majority of diabetic foot ulcers. Conversely, poor footwear is one of the most common triggers. Here's how to get footwear right:

Fit matters more than anything else. Have your feet measured every time you buy shoes — neuropathy can change your foot shape without you realizing it. Shop in the afternoon when feet are at their largest. The toe box should have enough room to wiggle all toes freely. Nothing should press, rub, or create friction at any point.
Therapeutic shoes designed for diabetic feet feature extra depth (to accommodate custom insoles and swollen feet), seamless interiors (no seams to rub against insensate skin), firm heel counters (for stability), and rocker-bottom soles (to reduce pressure on the forefoot).
Custom orthotics and insoles redistribute pressure across the entire bottom of your foot, reducing the concentrated pressure at bony prominences where ulcers typically form. According to a review in the International Journal of Molecular Sciences, individualized orthopedic shoe provision and custom insole treatment to adapt pressure distribution are core preventive measures.
Never go barefoot — not at home, not at the beach, not even for a quick trip to the bathroom at night. Keep supportive slippers by your bed. A single step on a sharp object you didn't see or feel could start the cascade toward an ulcer.
Check inside shoes before putting them on — run your hand around the interior to feel for pebbles, rough seams, or foreign objects. This takes three seconds and can prevent a wound.
Daily Foot Care Routine
Beyond daily inspection, a consistent foot care routine protects your skin barrier and reduces ulcer risk.

Washing: Wash feet daily with lukewarm water (test temperature with your elbow or a thermometer — never trust neuropathic feet to judge water temperature) and mild soap. Don't soak your feet for extended periods, as this can soften skin excessively and create opportunities for breakdown. Pat dry gently but thoroughly, especially between toes where moisture promotes fungal infections.
Moisturizing: Apply a good moisturizer to the tops and bottoms of your feet daily — but not between the toes, where moisture can promote fungal growth. Keeping skin hydrated prevents the dry cracks that become entry points for bacteria.
Nail care: Cut toenails straight across, filing sharp edges gently. Don't cut too short or dig into corners — this can cause ingrown toenails. If you can't see or reach your feet well, or if your nails are thick or difficult to cut, have a podiatrist handle nail care.
Callus management: Don't try to cut or shave calluses yourself. A podiatrist can safely reduce calluses using proper technique. Never use chemical callus removers or “bathroom surgery” — these are common causes of diabetic foot wounds.
Blood Sugar Control: The Foundation of Prevention
Everything else in this article builds on blood sugar management. High blood sugar damages nerves, impairs wound healing, weakens the immune system, and damages blood vessels. Controlling blood sugar won't reverse existing neuropathy, but it can slow its progression and give your body better resources for healing any wounds that do occur.

Studies consistently show that people with well-controlled diabetes (HbA1c below 7%) have significantly lower rates of foot ulcers and amputations compared to those with poor control. Work closely with your endocrinologist or primary care provider on your blood sugar management plan.
If you notice your neuropathy symptoms worsening or your feet losing more sensation, it may be a sign that blood sugar control needs to be tightened. Don't wait for a foot wound to motivate this conversation — have it proactively.
When a Wound Develops: What to Do
Despite your best prevention efforts, wounds can still happen. Knowing how to respond quickly can make the difference between a minor incident and a serious complication.
Immediate first aid: Clean the wound gently with saline or clean water. Apply a thin layer of antibiotic ointment. Cover with a sterile, non-adhesive bandage. Do not apply hydrogen peroxide, iodine, or alcohol directly to the wound — these can damage healing tissue.
Offload the area: Stop putting weight on the wound. This is critical. If the wound is on the bottom of your foot, you need to take pressure off that area for it to heal. Your doctor may prescribe a total contact cast, removable cast walker, or other offloading device. The evidence from Diabetes/Metabolism Research and Reviews confirms that pressure relief through offloading devices remains the mainstay of neuropathic ulcer treatment.
Seek medical care promptly — within 24 hours for any wound that breaks the skin. Don't adopt a “wait and see” approach with diabetic foot wounds. Early professional care dramatically improves outcomes.
Signs you need emergency care: Red streaks spreading from the wound, fever or chills, rapidly expanding redness or swelling, foul-smelling drainage, and darkening skin around the wound all require immediate medical attention.
Professional Wound Treatment
If a foot ulcer develops, professional treatment typically involves several key components.
Debridement: Removing dead tissue and callus from the wound to promote healing. This is typically done by a wound care specialist or podiatrist and may need to be repeated at regular intervals.
Infection management: If the wound is infected, antibiotics are prescribed based on culture results. Mild infections may be treated with oral antibiotics, while moderate to severe infections often require IV antibiotics and possibly hospitalization.
Vascular assessment: Your doctor should evaluate blood flow to your feet. If peripheral artery disease is limiting blood supply, vascular intervention (angioplasty or bypass surgery) may be needed before the wound can heal.
Advanced wound care: Modern wound treatment may include specialized dressings, negative pressure wound therapy (wound vac), growth factor application, skin substitutes, or hyperbaric oxygen therapy for wounds that aren't responding to standard care.
Multidisciplinary team: The best outcomes come from a team approach. The WoundSource review emphasizes that multidisciplinary teams — including podiatrists, endocrinologists, and vascular surgeons — improve ulcer healing rates and amputation prevention.
Building Your Prevention Team
Preventing diabetic foot ulcers isn't a solo project. Building the right team of professionals and knowing how often to see them is part of the strategy.

Podiatrist: See a podiatrist at least once a year for a comprehensive foot exam (more often if you have moderate to high risk factors). They handle callus management, nail care, footwear recommendations, and early problem detection.
Endocrinologist or primary care provider: Regular diabetes management visits to optimize blood sugar, blood pressure, and cholesterol — all of which affect foot health.
Neurologist: Periodic assessment of neuropathy progression. Knowing when to see a neurologist helps you stay ahead of changing nerve function.
Certified diabetes educator: These specialists can teach you foot care techniques, help with blood sugar management strategies, and connect you with insurance resources for therapeutic footwear and supplies.
Vascular specialist: If you have known peripheral artery disease or signs of poor circulation (slow-healing wounds, absent foot pulses, leg pain with walking), a vascular assessment is important.
Reducing Your Risk: A Complete Checklist
Here's everything you can do to reduce your risk of developing a diabetic foot ulcer, distilled into actionable daily, weekly, and ongoing habits:
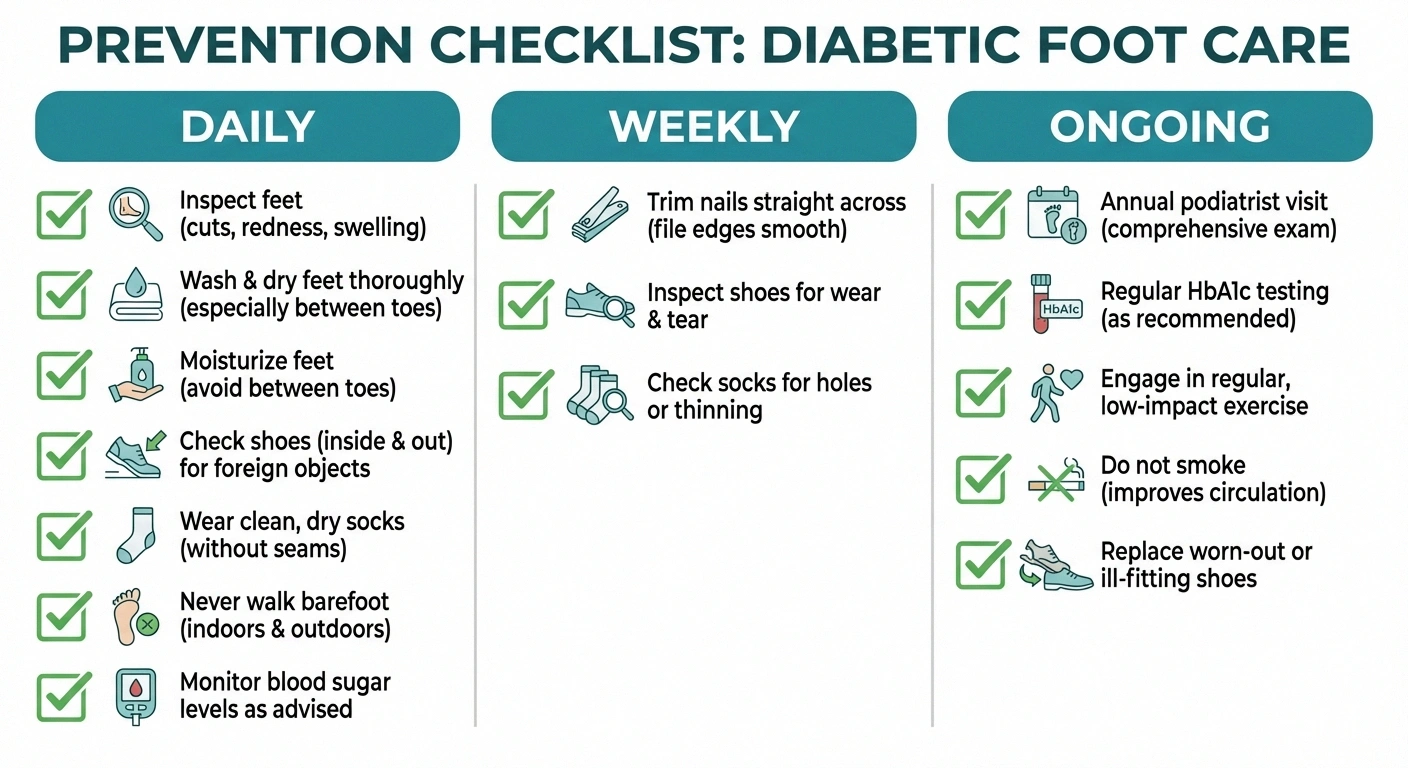
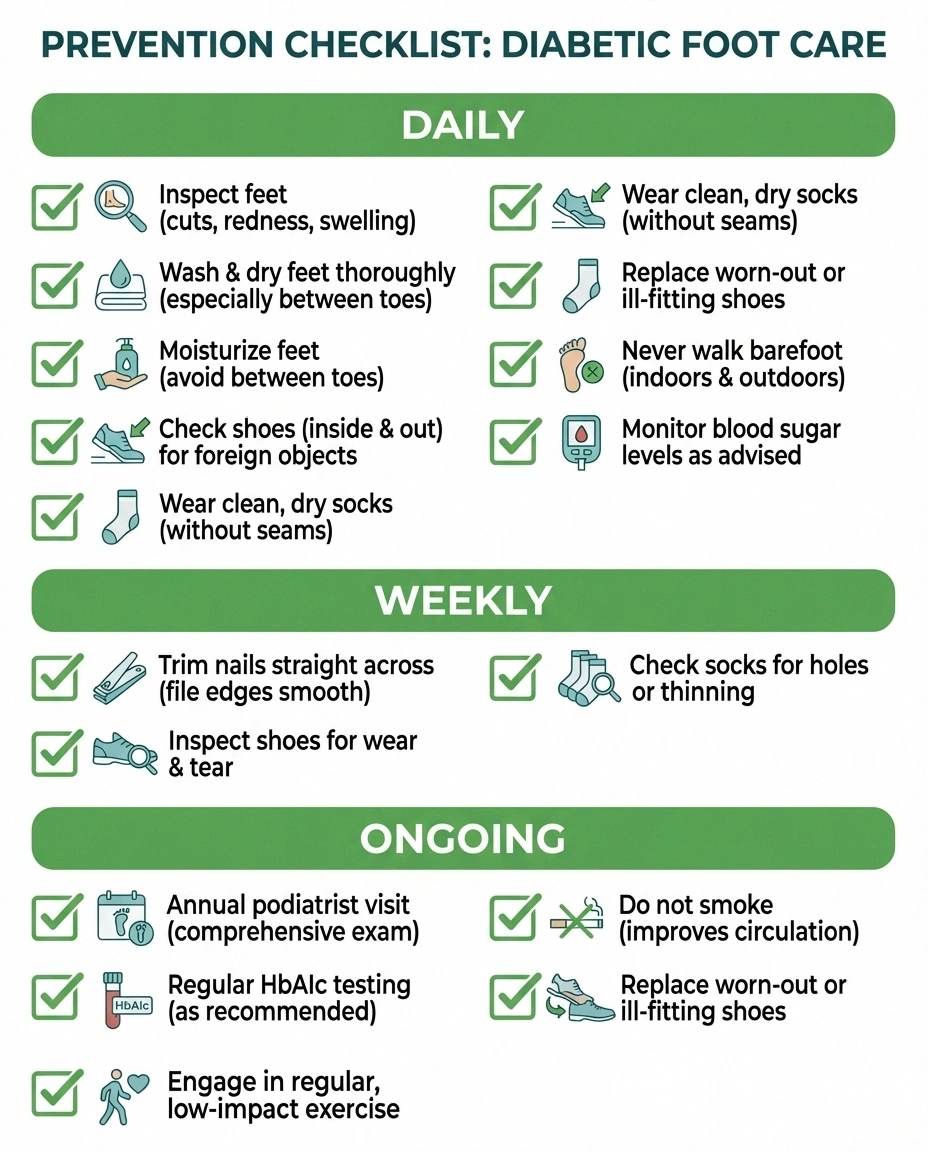
Daily:
- Inspect both feet thoroughly in good lighting
- Wash and dry feet carefully
- Moisturize (not between toes)
- Check shoes before putting them on
- Wear clean, dry, non-binding socks
- Never walk barefoot
- Monitor blood sugar
Weekly:
- Trim toenails (or schedule professional care)
- Inspect shoes for wear, loose linings, or foreign objects
- Check that socks have no holes or rough seams
Ongoing:
- Annual comprehensive foot exam by a podiatrist
- Regular HbA1c testing (target below 7% or as recommended by your doctor)
- Regular exercise to improve circulation
- Don't smoke — smoking dramatically reduces blood flow to the feet
- Replace shoes when they show wear or no longer fit properly
- Report any foot changes to your healthcare team promptly
Frequently Asked Questions
Can diabetic foot ulcers be prevented?
Yes, the majority of diabetic foot ulcers are preventable with consistent daily foot care, proper footwear, blood sugar control, and regular professional foot exams. Studies show that patient education combined with regular podiatric care significantly reduces ulcer rates. Prevention isn't about doing one big thing — it's about consistently doing many small things every day.
How long do diabetic foot ulcers take to heal?
Healing time varies widely depending on ulcer severity, blood flow, infection status, and how well blood sugar is controlled. Superficial ulcers may heal in a few weeks with proper care. Deeper ulcers can take 3 to 6 months or longer. Some ulcers become chronic and require months of specialized wound care. The key factor affecting healing time is offloading — keeping weight off the wound.
Why do diabetic foot ulcers lead to amputation?
Amputation happens when an ulcer becomes severely infected and the infection spreads to bone or deep tissue, when blood supply is too poor to support healing, or when tissue death (gangrene) progresses beyond what can be surgically cleaned. Early treatment of ulcers, infection control, and vascular assessment reduce amputation risk dramatically. Most amputations are preceded by an ulcer that could have been caught and treated earlier.
Does Medicare cover diabetic shoes?
Yes, Medicare Part B covers therapeutic shoes and custom insoles for people with diabetes under the Therapeutic Shoe Bill. You need a prescription from your treating physician and the shoes must be fitted by a podiatrist, orthotist, prosthetist, or pedorthist. Coverage typically includes one pair of custom-molded shoes or one pair of depth shoes plus three pairs of custom insoles per calendar year.
Should I see a podiatrist even if my feet look fine?
Absolutely. If you have diabetes with neuropathy, annual podiatric exams are recommended even when your feet appear healthy. A podiatrist can detect subtle changes you might miss — early callus patterns, foot deformity progression, reduced blood flow, and other risk factors that indicate your prevention plan needs adjustment. Think of it like a dental checkup — prevention is easier than treatment.
What are the best socks for diabetic neuropathy?
Look for diabetic socks that have no seams (or flat seams) to prevent friction, moisture-wicking material to keep feet dry, a non-binding top that doesn't restrict circulation, light padding at pressure points, and white or light color (so you can spot drainage from an unnoticed wound). Avoid socks with tight elastic bands that can reduce blood flow.
Your Feet Are Worth Fighting For
I know that adding foot care to an already demanding diabetes management routine can feel overwhelming. But here's the reality: the daily time investment is minutes, and the payoff is keeping your feet healthy and functional for years to come. Every reader who has written to me after a foot ulcer says the same thing — “I wish I had taken prevention more seriously before this happened.”
You have the knowledge now. Make the daily foot check as automatic as brushing your teeth. Get the right shoes. See your podiatrist. And if something doesn't look right, don't wait. Your feet carried you through life before neuropathy, and with proper care, they'll keep carrying you.
For more on protecting your overall nerve health, explore our complete guide to living well with neuropathy.


