If you've ever come home from a doctor's appointment with a fistful of new words and a vague idea what most of them meant, this article is for you. I've lost count of how many times I've sat with someone in our support group, helping them piece together what their neurologist actually said. Half the battle with neuropathy is just learning the language.
This is a plain-English glossary of the terms you're most likely to encounter — on test reports, prescription labels, support forums, and in the literature. I've organized it A to Z so you can scan it quickly when something specific comes up. For the most important terms, I've linked out to deeper articles on this site where we cover them in full.
If a word you're looking for isn't here, send me an email and I'll add it. This is a living document.
How to Use This Glossary
Each entry has a one-line definition first, then a sentence or two of context. When the term is something you might see on a lab order, prescription, or imaging report, I've added a “Where you'll see it” note. When we have a full article on the topic, I've linked it.
🔎 Research Says
Studies of patient comprehension after neurology appointments consistently show that patients remember less than 50% of what was said, and misremember a meaningful portion of the rest. Writing terms down during the visit and looking them up afterward is one of the most evidence-supported “patient activation” strategies in chronic disease care.
80+
Terms Defined
From allodynia to Wallerian degeneration — the working vocabulary of neuropathy, in plain English.
How to Use This Page
Bookmark this page. Pull it up after appointments to decode unfamiliar terms. Use Ctrl+F (or Cmd+F) to search any word quickly. We've linked the most important terms to deeper articles where we cover them in full.
I've kept the entries patient-readable. If you need the technical definition for a class assignment or a clinical chart note, the National Institute of Neurological Disorders and Stroke (NINDS) glossary at ninds.nih.gov is the federal standard. This page is meant for the rest of us.
A
Allodynia — Pain from something that shouldn't hurt: a bedsheet brushing your foot, a light breeze, the weight of a sock. The nerve is misinterpreting normal touch as pain. Full article on allodynia.
Easy to Confuse
Neuralgia (pain along one nerve), neuropathy (any nerve disease), radiculopathy (nerve root irritation at the spine), and peripheral arterial disease (blood vessel problem mimicking neuropathy) all produce overlapping symptoms but require very different workups. Don't let the words be used interchangeably with your doctor.
Five Categories of Terms You'll See Most Often
Symptoms
Paresthesia, allodynia, dysesthesia, hyperalgesia, numbness
Anatomy
Axon, myelin, brachial plexus, sural nerve, peripheral nervous system
Diagnosis & Tests
EMG, NCS, skin punch biopsy, IENFD, QSART
Conditions
CIDP, GBS, CIPN, small fiber, vasculitic, autonomic, CMT
Treatments
Gabapentin, pregabalin, IVIG, plasmapheresis, TENS, ALA, benfotiamine
Alpha-Lipoic Acid (ALA) — A naturally-occurring antioxidant that has been studied as a supplement for diabetic neuropathy, especially in Europe. Some randomized trials have shown modest benefit. Full article on ALA.
Amyloid Neuropathy (ATTR) — A rare form of neuropathy caused by abnormal protein deposits (amyloid) accumulating in nerves and other tissues. Increasingly treatable with newer medications. Full article on amyloid neuropathy.
Antiganglioside Antibodies — Antibodies that target gangliosides — molecules found on nerve cell membranes. Their presence helps diagnose certain immune-mediated neuropathies including Guillain-Barré syndrome and multifocal motor neuropathy.
Apheresis — A procedure that separates blood into its components and removes one of them. Plasmapheresis is one type. Full article on plasma exchange.
Autonomic Neuropathy — Damage to the nerves that control automatic body functions: blood pressure, heart rate, digestion, sweating, bladder function, sexual response. Often coexists with the more familiar sensory neuropathy. Full article on autonomic neuropathy.
Axon — The long thin fiber that carries the electrical signal from a nerve cell body to its target. In axonal neuropathy, this is what's damaged.
B
Benfotiamine — A fat-soluble form of vitamin B1 (thiamine) that's better absorbed than the standard form. Often taken by people with diabetic neuropathy. Full article on benfotiamine.
Biologics — A class of medications made from living organisms (often antibodies). Examples include infliximab, adalimumab, and rituximab. Used in autoimmune diseases including some neuropathies.
Biopsy (skin or nerve) — A small tissue sample taken for laboratory examination. Skin punch biopsy is the gold-standard test for small fiber neuropathy. Sural nerve biopsy is used in select cases of suspected vasculitic or atypical neuropathy.
Brachial Plexus — The network of nerves at the shoulder that supplies the arm. Brachial plexus neuropathy (Parsonage-Turner syndrome) causes sudden severe shoulder pain followed by arm weakness.
C
Capsaicin Cream — A topical pain reliever derived from chili peppers. Depletes a pain-signaling molecule in skin nerves. Full article on capsaicin.
Carpal Tunnel Syndrome — Compression of the median nerve at the wrist. The most common entrapment neuropathy. Causes tingling and numbness in the thumb, index, and middle fingers.
Causalgia — Severe burning pain following a nerve injury. Now usually called complex regional pain syndrome (CRPS) Type II.
Central Sensitization — A state in which the central nervous system has become “wound up” and amplifies pain signals. Common in long-standing neuropathy. Full article on central sensitization.
Charcot Foot — Progressive deformity of the foot in long-standing neuropathy, especially diabetic. Bones weaken and joints collapse painlessly because of lost sensation.
Charcot-Marie-Tooth Disease (CMT) — The most common inherited (genetic) neuropathy. Slowly progressive, often presenting with foot drop and high-arched feet in adolescence or early adulthood.
Chemotherapy-Induced Peripheral Neuropathy (CIPN) — Nerve damage from cancer treatment. Most commonly caused by platinum drugs, taxanes, vinca alkaloids, and bortezomib. Full article on CIPN.
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) — A treatable autoimmune neuropathy with progressive weakness over weeks to months. Often called the “chronic cousin” of Guillain-Barré. Full article on CIDP.
Complex Regional Pain Syndrome (CRPS) — Severe burning pain, color and temperature changes, and swelling in a limb after an injury or surgery. Type I has no clear nerve injury; Type II follows a known nerve injury (formerly called causalgia).
D
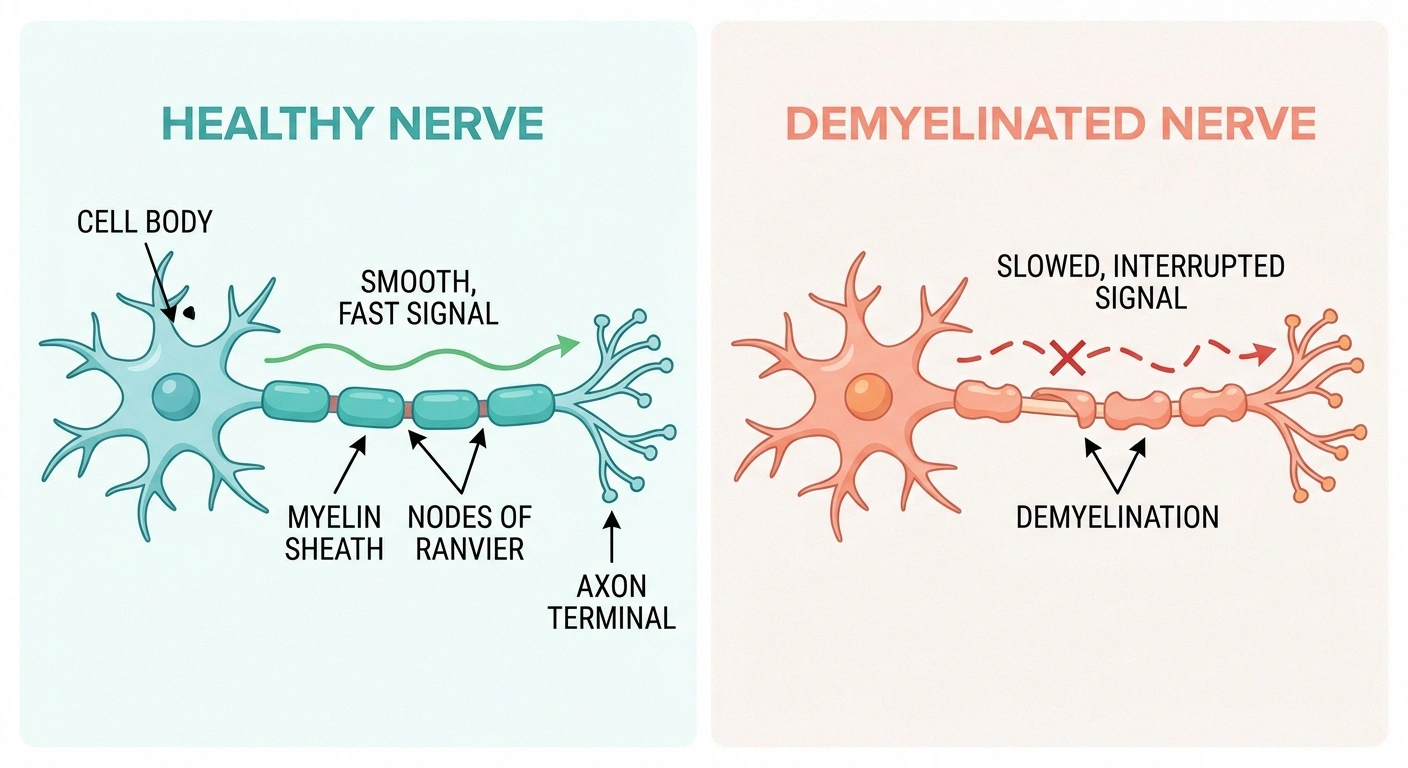
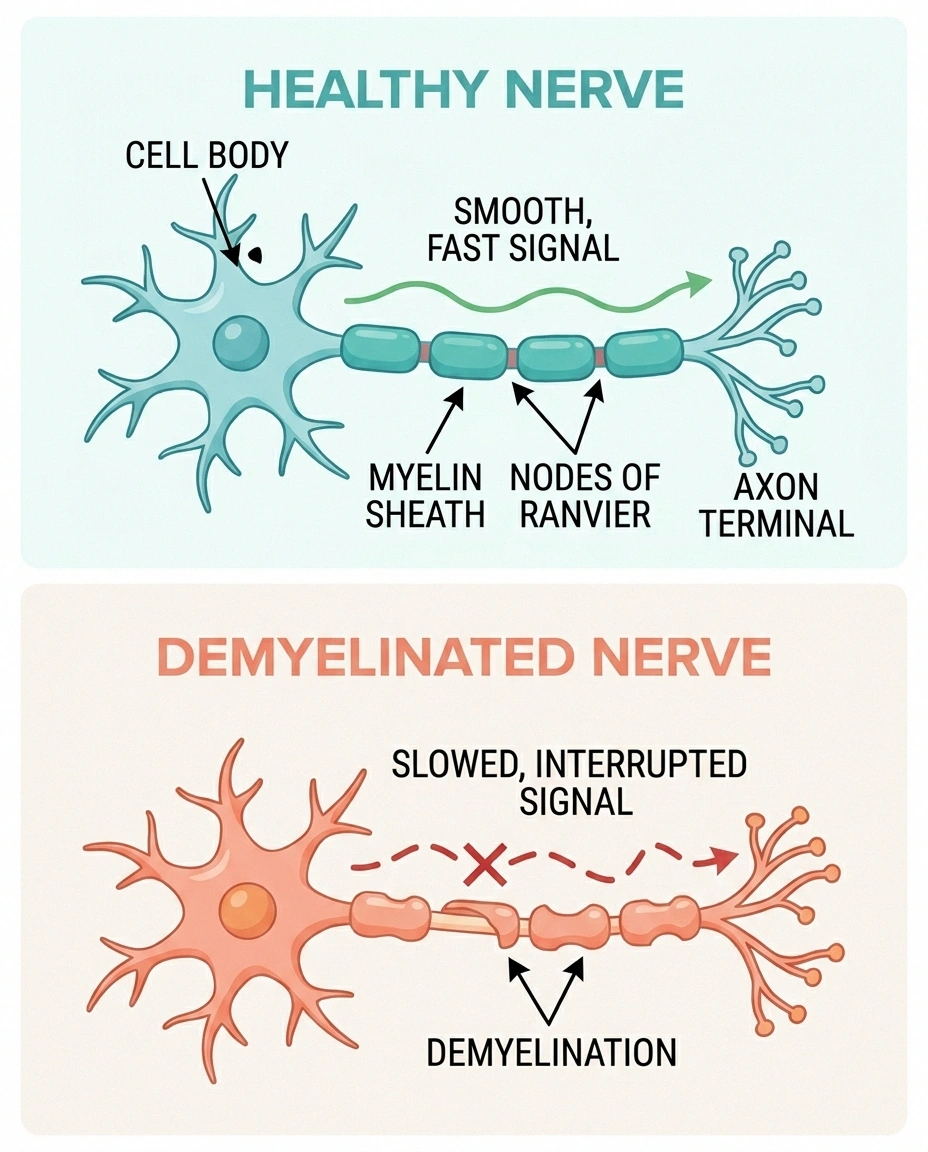
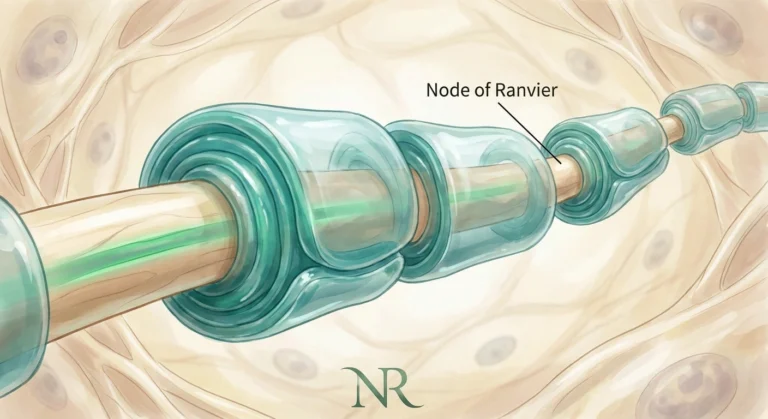
Demyelination — Damage to the myelin sheath — the protective insulation around nerve fibers. Slows nerve signal transmission. Full article on demyelinating vs axonal.
Diabetic Neuropathy — Nerve damage caused by chronically elevated blood sugar. The single most common cause of neuropathy worldwide. Full article on diabetic neuropathy.
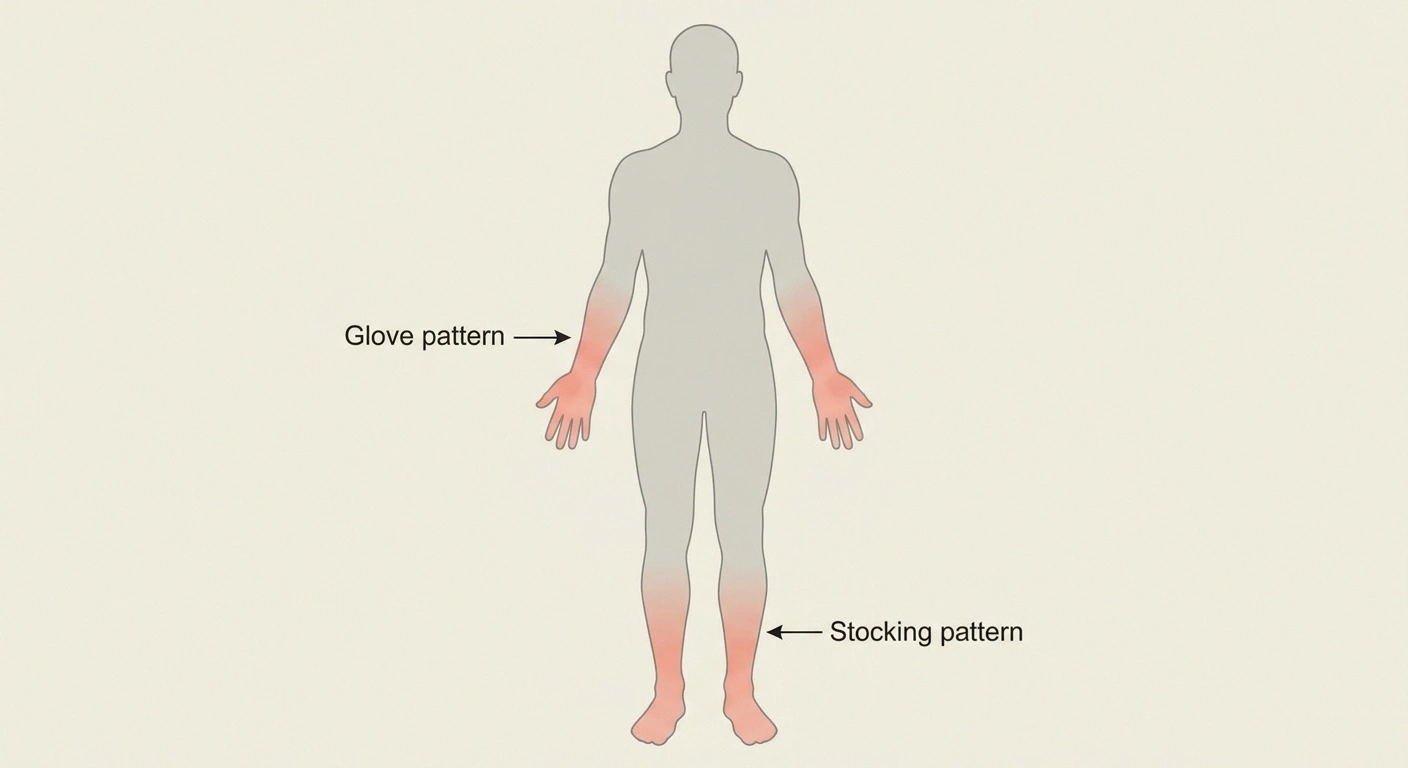
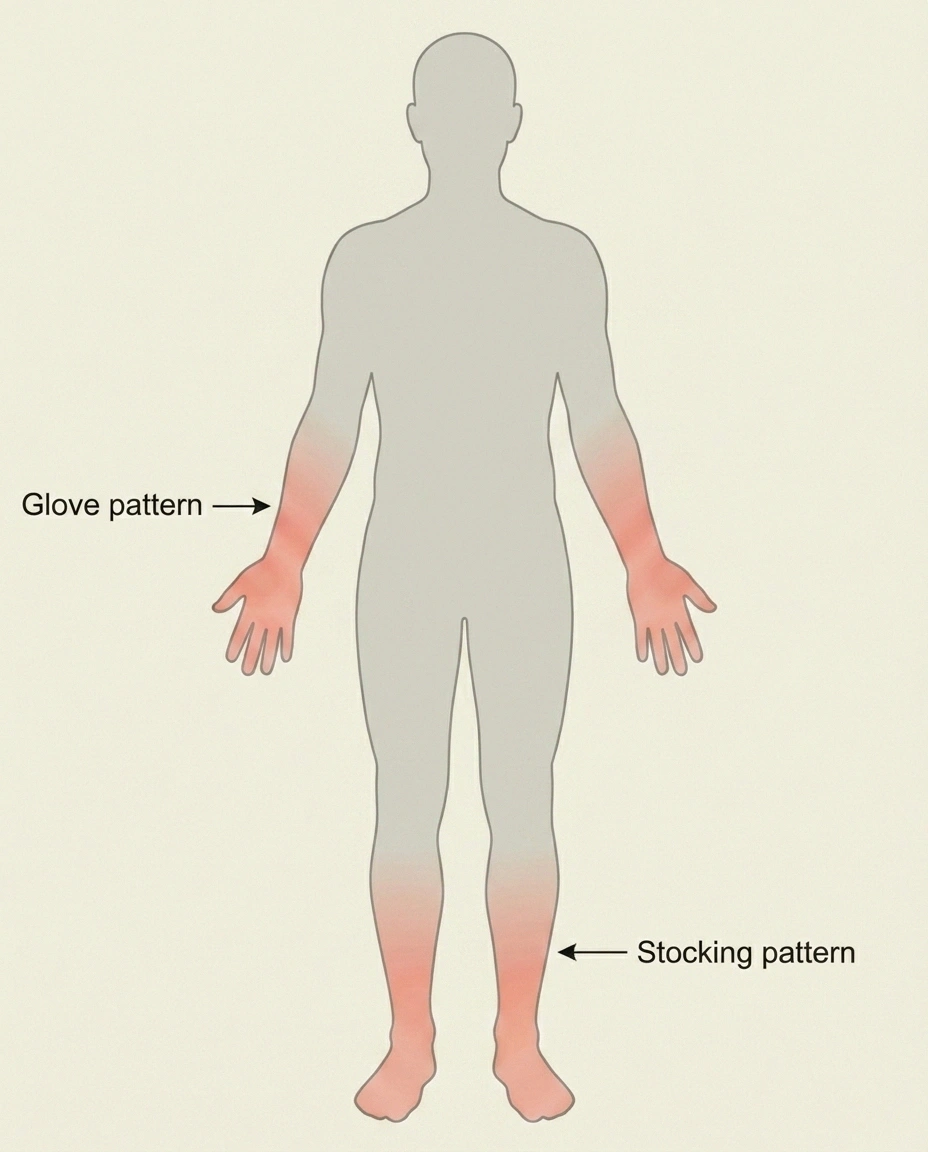
Distal Symmetric Polyneuropathy (DSPN) — The classic “stocking-and-glove” pattern: tingling and numbness that starts in the toes and feet and slowly creeps up. Most common form of polyneuropathy.
Dysesthesia — An unpleasant abnormal sensation, whether spontaneous or evoked. Burning, electric, crawling — the patient knows it's not a normal feeling but can't always describe it precisely.
E
EMG (Electromyography) — A test that measures the electrical activity of muscles. Often paired with nerve conduction studies. Full article on EMG/NCS.
Entrapment Neuropathy — A nerve compressed at a specific location: carpal tunnel (median nerve at wrist), cubital tunnel (ulnar nerve at elbow), tarsal tunnel (tibial nerve at ankle), peroneal at the fibular head, and others.
Erythromelalgia — A rare condition causing intense burning, redness, and warmth in the hands and feet, often triggered by warmth or activity. Sometimes confused with neuropathy.
F
Fasciculation — A small involuntary muscle twitch visible under the skin. Common, usually benign in isolation, but can occur in motor neuron disease and some neuropathies.
Foot Drop — Inability to lift the front of the foot, causing the toes to drag during walking. Most often from peroneal nerve injury or L5 radiculopathy.
G
Gabapentin — One of the two most commonly prescribed medications for neuropathic pain (the other is pregabalin). Originally developed for seizures. Full article on gabapentin.
Ganglion / Ganglionopathy — A ganglion is a cluster of nerve cell bodies. Sensory ganglionopathy is damage at the dorsal root ganglion (the cluster near the spine that handles sensory input), producing severe sensory ataxia.
Guillain-Barré Syndrome (GBS) — An acute autoimmune neuropathy that causes rapidly progressive weakness, sometimes leading to paralysis within days. Often follows an infection. Treated with plasma exchange or IVIG.
H
Hereditary Neuropathy — A neuropathy caused by inherited genetic mutations. CMT is the most common; hereditary neuropathy with liability to pressure palsies (HNPP) and familial amyloid neuropathy are others.
Hyperalgesia — Increased pain from a stimulus that normally produces pain — for example, a pinprick that hurts much more than expected.
Hyperesthesia — Increased sensitivity to non-painful stimulation. Light touch feels intensified.
Hyporeflexia / Areflexia — Reduced or absent reflexes. A common physical exam finding in polyneuropathy and a defining feature of GBS.
I
Idiopathic Neuropathy — A neuropathy with no identified cause despite a thorough workup. Roughly 20–30% of polyneuropathies remain idiopathic. Full article on idiopathic neuropathy.
Intraepidermal Nerve Fiber Density (IENFD) — The measurement obtained from a skin punch biopsy. Counts the small unmyelinated fibers in the skin. The diagnostic test for small fiber neuropathy.
IVIG (Intravenous Immunoglobulin) — Pooled antibodies from healthy donors, given IV to modulate the immune system. First-line treatment for many immune-mediated neuropathies. Full article on IVIG.
L
Length-Dependent Neuropathy — A neuropathy where the longest nerves are affected first, which is why feet usually go before hands. Most polyneuropathies follow this pattern. Full article on length-dependent neuropathy.
Lhermitte's Sign — An electric-shock sensation down the spine and into the limbs when the neck is flexed forward. More common in MS than in peripheral neuropathy, but can occur in cervical spine disease and certain chemotherapy-induced neuropathies.
M
MGUS (Monoclonal Gammopathy of Undetermined Significance) — An abnormal protein in the blood that can sometimes be associated with neuropathy. Most cases never progress to malignancy but warrant ongoing monitoring.
Mononeuritis Multiplex — Damage to multiple individual nerves at the same time, often asymmetric. Classic in vasculitis. Different from polyneuropathy, which is symmetric.
Mononeuropathy — Damage to a single nerve, usually from compression or injury. Carpal tunnel is a mononeuropathy.
Motor Neuropathy — Predominantly affects motor (movement) nerves. Causes weakness rather than sensory symptoms. Full article on motor vs sensory.
Myelin — The fatty sheath that insulates many nerve fibers and speeds signal transmission. Full article on myelin.
N
Nerve Conduction Study (NCS) — Measures how fast and how strongly an electrical signal travels along a nerve. Slow speed suggests demyelination; small amplitude suggests axonal damage. Often paired with EMG.
Neuralgia — Pain along the course of a nerve, typically from injury or irritation of that nerve.
Neuropraxia — Mildest grade of nerve injury. The nerve is bruised or temporarily compressed but the structure is intact. Recovery is usually full.
Neurotmesis — Most severe grade of nerve injury. The nerve is completely cut. Usually requires surgical repair.
Numbness — Reduced or absent sensation. Often described as feeling “dead” or “wooden.”
O
Onion Bulb Formation — A microscopic finding in chronic demyelinating neuropathies. Repeated cycles of damage and repair create concentric rings around nerve fibers, like an onion cross-section.
P
Paresthesia — Tingling, prickling, “pins and needles,” or crawling sensations. The hallmark symptom of small fiber neuropathy and many other types.
Peripheral Nervous System (PNS) — All the nerves outside the brain and spinal cord. Neuropathy by definition affects the PNS, distinguishing it from central nervous system disorders like MS.
Plasmapheresis (Plasma Exchange) — A procedure that removes antibodies and immune molecules from the bloodstream. First-line treatment for severe immune-mediated neuropathies. Full article on plasmapheresis.
Polyneuropathy — Damage to many peripheral nerves simultaneously, usually symmetric. The classic “stocking-and-glove” pattern.
Post-Herpetic Neuralgia (PHN) — Chronic burning or stabbing pain that persists after a shingles outbreak has healed. Full article on PHN.
Pregabalin (Lyrica) — One of the two most commonly prescribed neuropathic pain medications (the other is gabapentin). Full article on Lyrica.
Proprioception — Your sense of where your body is in space without looking. When proprioception is damaged, balance and coordination suffer dramatically. Full article on proprioception loss.
Q
QSART (Quantitative Sudomotor Axon Reflex Test) — A test of small-fiber autonomic function that measures sweating. Used to diagnose small fiber neuropathy and autonomic dysfunction.
R
Radiculopathy — Damage or irritation of a nerve root as it exits the spine. Often confused with peripheral neuropathy. Sciatica is the most familiar example.
Refractory Neuropathy — Neuropathy that has not responded to standard first-line treatments. Generally a signal to broaden the workup or try a different therapeutic approach.
S

Sensorimotor Neuropathy — Affects both sensory and motor fibers. The most common pattern in polyneuropathy.
Sensory Ataxia — Loss of balance and coordination from sensory nerve damage rather than from a brain or inner ear problem. Tends to worsen in the dark or with eyes closed.
Small Fiber Neuropathy (SFN) — Damage to the smallest unmyelinated nerve fibers. Causes burning, tingling, and autonomic symptoms with normal standard nerve conduction studies. Diagnosed by skin biopsy. Full article on SFN.
Stocking-and-Glove Distribution — The classic length-dependent pattern of polyneuropathy: symptoms in the area covered by socks and gloves.
Sural Nerve — A purely sensory nerve in the lower leg often used for nerve biopsies and as a target for nerve conduction studies. Easy to access and minimally consequential when sampled.
Sympathetic Nerves — One arm of the autonomic nervous system. Activates “fight or flight” responses. Damaged in some autonomic neuropathies.
T
TENS (Transcutaneous Electrical Nerve Stimulation) — A small device that delivers mild electrical pulses through skin electrodes to mask pain signals. Full article on TENS.
Thalamus — A brain region that relays sensory information. Some chronic neuropathic pain involves changes in thalamic processing.
Trigeminal Neuralgia — Sudden, severe, electric-shock-like facial pain caused by irritation of the trigeminal (5th cranial) nerve. Full article on trigeminal neuralgia.
Tricyclic Antidepressants (TCAs) — An older class of antidepressants used at low doses for neuropathic pain. Amitriptyline and nortriptyline are common examples. Full article on amitriptyline.
V
Vasculitic Neuropathy — Nerve damage from inflammation of the small blood vessels that feed nerves. Often presents as mononeuritis multiplex. Full article on vasculitic neuropathy.
Vibratory Sensation — The ability to feel vibrations, tested with a tuning fork. One of the first sensory modalities lost in length-dependent neuropathy.
W
Wallerian Degeneration — The process by which the part of a nerve fiber distal to (downstream of) an injury breaks down and is reabsorbed. Sets the stage for nerve regeneration if conditions allow.
Wasting (Muscle Atrophy) — Visible thinning of muscles from disuse or denervation. A late finding in long-standing motor neuropathy.
How These Terms Connect

Most patients don't get every term thrown at them at once. They show up in waves. The first appointment usually introduces a handful — paresthesia, polyneuropathy, EMG, and a few medication names. Later visits add more — small fiber neuropathy, IVIG, plasma exchange, central sensitization. By the time you've been navigating neuropathy for a year, you'll know more medical vocabulary than most people learn in a decade.
A Five-Step Strategy For Decoding Your Visits
Bring a notebook and pen
Phones are awkward. A small notebook signals that you're paying attention.
Write down every unfamiliar word
Including diagnosis names, test abbreviations, and medication names. Ask for spellings if needed.
Look them up in this glossary
Most appointment vocabulary will be here. For deeper coverage, follow the linked articles.
Bring questions to the next visit
“You said ‘demyelinating' last time — what does that mean for my treatment plan?”
Build your personal vocabulary file
After a year of doing this, most patients can read their own chart notes confidently.
If a doctor uses a word that you don't recognize, please — write it down and ask them to spell it. There's nothing embarrassing about that. The same goes for medication names, test names, and diagnoses. Half my early appointments were spent nodding politely at words I didn't understand. Once I started writing them down and looking them up later, I felt like a different patient at the next visit.
For the foundational terms — what neuropathy is, the stages it progresses through, what kinds exist — I recommend starting with our stages of neuropathy guide and our peripheral neuropathy overview. They cover the same vocabulary in deeper context.
Frequently Asked Questions
What's the difference between neuralgia and neuropathy?
Neuralgia is pain along the path of a specific nerve, usually from local injury or irritation. Examples include trigeminal neuralgia and post-herpetic neuralgia. Neuropathy is broader — any disease or dysfunction of one or more peripheral nerves, which may or may not include pain. You can have neuropathy without neuralgia (numbness without pain) and you can have neuralgia without classical polyneuropathy.
Is paresthesia the same as neuropathy?
No. Paresthesia is a symptom — tingling, prickling, or pins-and-needles. It's the most common symptom of small fiber neuropathy, but it can also be caused by a temporarily compressed nerve, anxiety, hyperventilation, certain medications, or vitamin deficiencies. Persistent or progressive paresthesia warrants a workup; brief paresthesia from a leg falling asleep does not.
What's the difference between polyneuropathy and mononeuropathy?
Polyneuropathy affects many peripheral nerves at once, usually symmetrically — the classic stocking-and-glove pattern. Mononeuropathy affects a single nerve, usually from compression or injury — carpal tunnel syndrome is the most common example. Mononeuritis multiplex is something different again — multiple individual nerves damaged at the same time, but asymmetrically, classically in vasculitis.
What does “axonal” versus “demyelinating” mean on my EMG report?
The two findings describe what part of the nerve is damaged. Axonal damage affects the long fiber that carries the signal; demyelinating damage affects the insulation around it. The distinction matters for diagnosis and treatment — demyelinating neuropathies are more often immune-mediated and often respond to immunotherapy, while axonal neuropathies are more often metabolic or toxic and tend to recover more slowly.
What does “length-dependent” mean?
It means the longest nerves are affected first. The longest nerves in your body are the ones that travel from the lower spine to the toes — that's why most polyneuropathies start in the feet and creep upward over time. As the disease progresses to involve nerves that supply the fingertips, the pattern produces the familiar stocking-and-glove distribution.
What is a skin punch biopsy and why might my neurologist order one?
A skin punch biopsy is a small tissue sample (3 millimeters wide) taken usually from the calf or thigh under local anesthesia. The lab counts the small nerve fibers in that sample to measure intraepidermal nerve fiber density (IENFD). It's the gold-standard test for small fiber neuropathy because standard nerve conduction studies don't measure small fibers. If your symptoms suggest SFN — burning, tingling, autonomic complaints — but standard testing is normal, this is the next step.
Where can I find a more technical glossary of neurological terms?
The National Institute of Neurological Disorders and Stroke (NINDS) maintains a comprehensive Glossary of Neurological Terms at ninds.nih.gov. It's the federal standard reference. The Foundation for Peripheral Neuropathy also publishes a shorter neuropathy-specific glossary. Both are good complements to the patient-friendly version on this page.