If you're living with lupus and have started noticing tingling, numbness, or burning pain in your hands and feet, you're not imagining things — and you're not alone. Peripheral neuropathy is a recognized complication of systemic lupus erythematosus (SLE), affecting an estimated 3-28% of people with lupus depending on the study and diagnostic criteria used.
What makes lupus neuropathy particularly frustrating is that it can be hard to pin down. The symptoms overlap with lupus itself, with medication side effects, and with other conditions. Many people go months or years before the nerve damage is properly identified and treated. This guide explains exactly how lupus damages your peripheral nerves, what symptoms to watch for, how it's diagnosed, and what treatment options are available.
How Lupus Damages Your Nerves
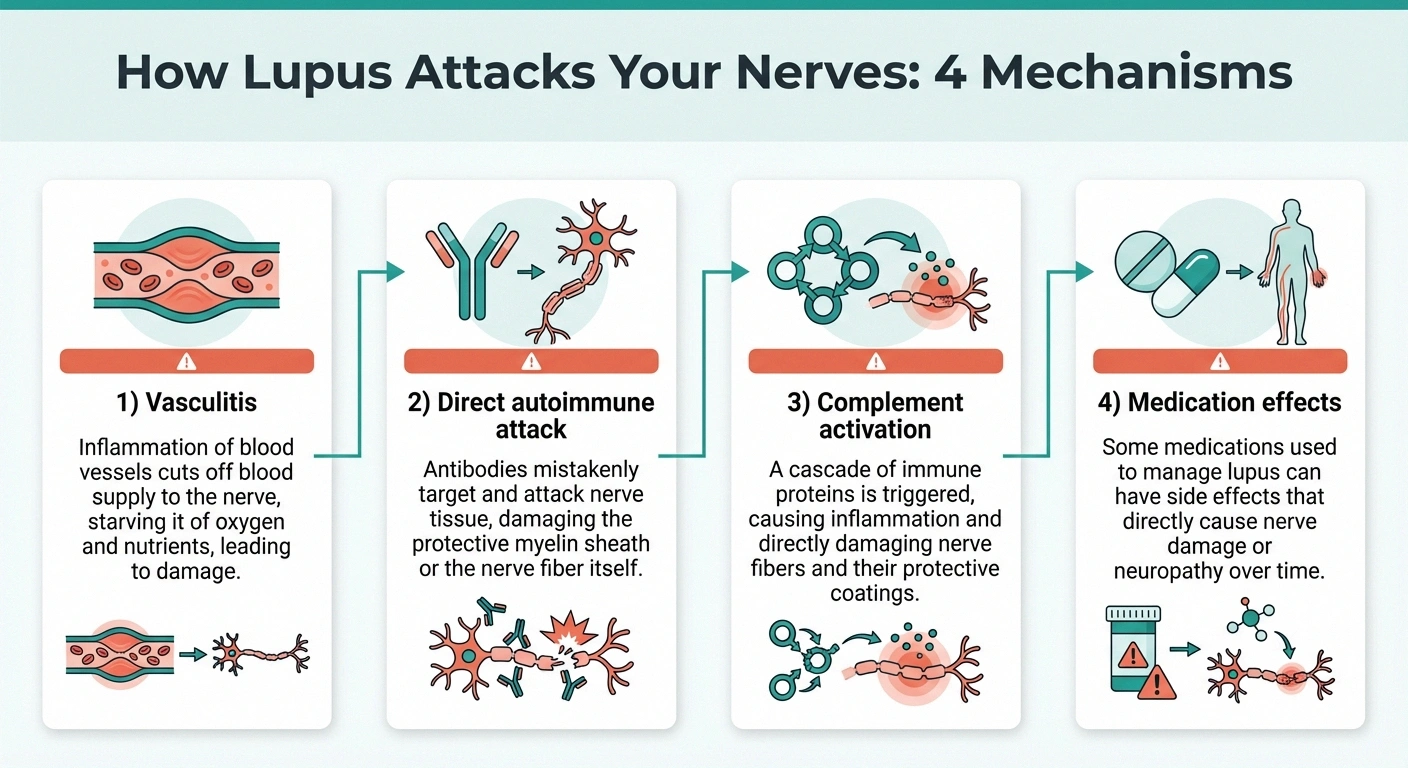
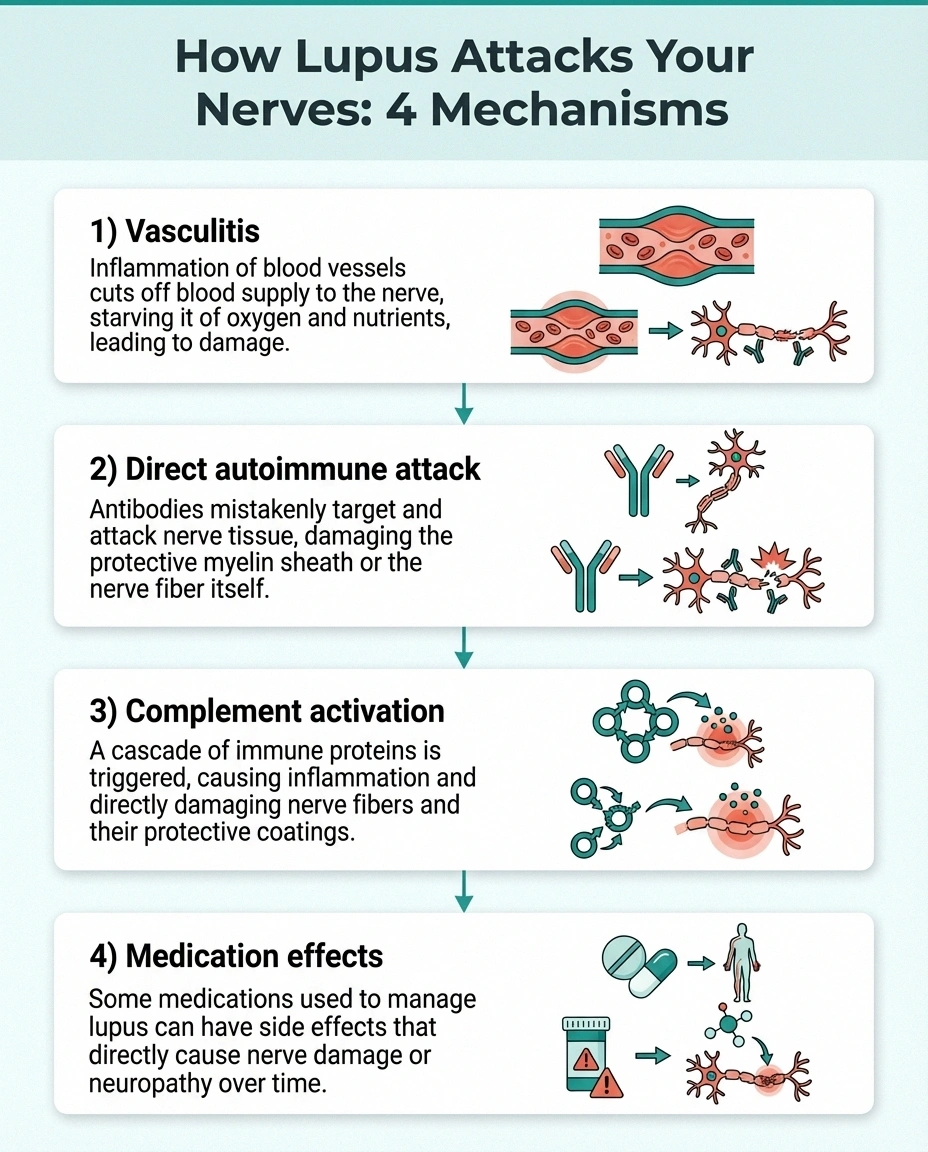
Lupus is an autoimmune disease — your immune system mistakenly attacks healthy tissue throughout your body. When this attack reaches your peripheral nervous system, several mechanisms can cause nerve damage.
Prevalence studies range from 3-28% depending on diagnostic methods. Sensitive testing (nerve conduction studies + skin biopsy) detects higher rates of subclinical nerve damage.
Vasculitis (blood vessel inflammation). The most common mechanism. Lupus can inflame the small blood vessels that supply nutrients and oxygen to your peripheral nerves. When these tiny blood vessels become inflamed or blocked, the nerves they feed are starved of oxygen and begin to deteriorate. This is called vasculitic neuropathy, and it's the same process that drives vasculitic neuropathy from other autoimmune conditions.
Direct autoimmune attack. Lupus antibodies — specifically anti-neuronal antibodies and anti-ganglioside antibodies — can directly target nerve tissue. These antibodies bind to components of the nerve cell, triggering inflammation and damage at the nerve fiber itself. A 2020 inception cohort study published in Arthritis & Rheumatology confirmed that autoimmune-mediated nerve damage is a distinct mechanism separate from vasculitis in lupus patients.
Complement system activation. Lupus activates the complement system — a group of immune proteins that normally fight infections but in autoimmune disease can damage your own tissues. Complement deposits have been found in the peripheral nerves of lupus patients, contributing to nerve fiber destruction.
Medication-related nerve damage. Some medications used to treat lupus can themselves cause neuropathy. Long-term corticosteroid use may contribute to nerve problems, and certain immunosuppressive drugs have neurotoxic potential. This creates a diagnostic challenge — is the neuropathy from the lupus or from the treatment?
Types of Neuropathy Seen in Lupus
Lupus doesn't cause just one type of neuropathy — it can affect your peripheral nerves in several distinct patterns, each with different symptoms and implications.
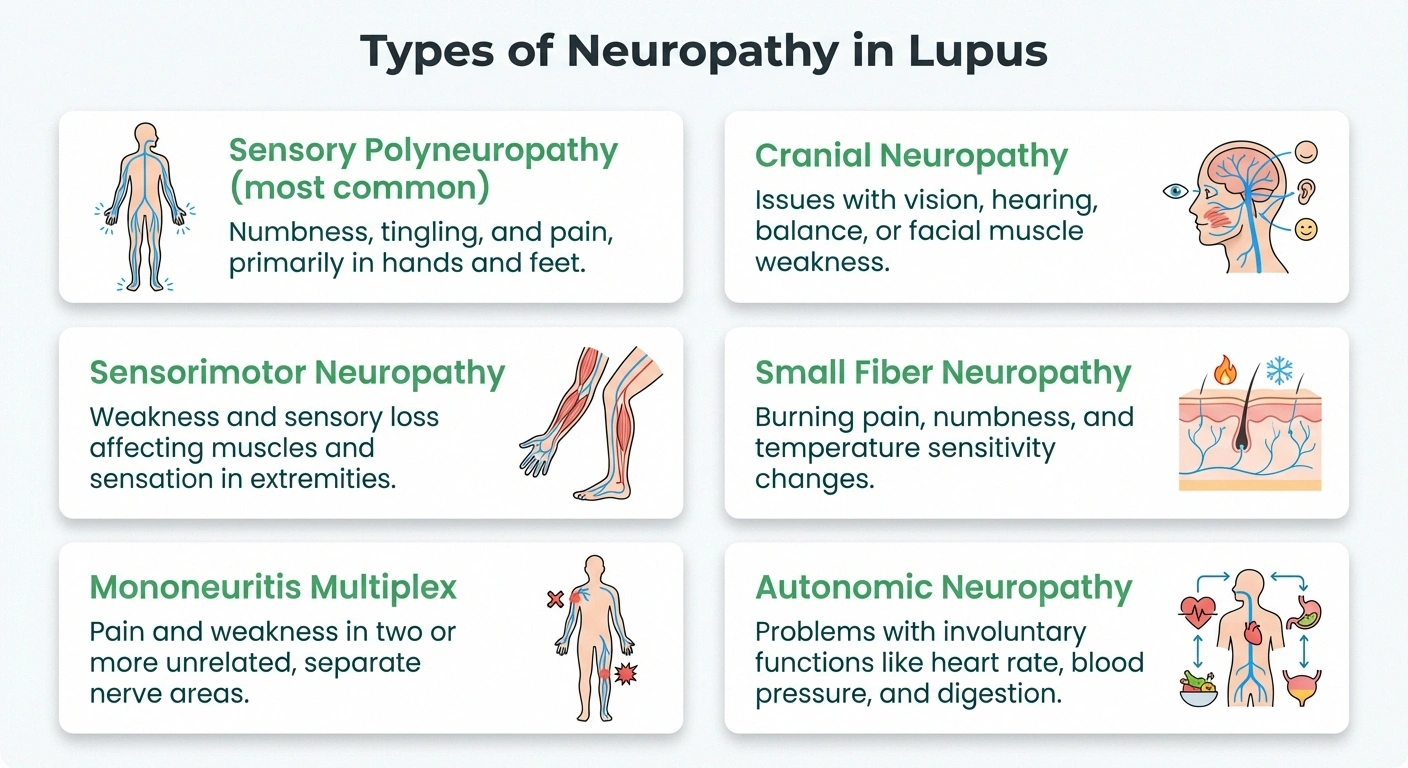
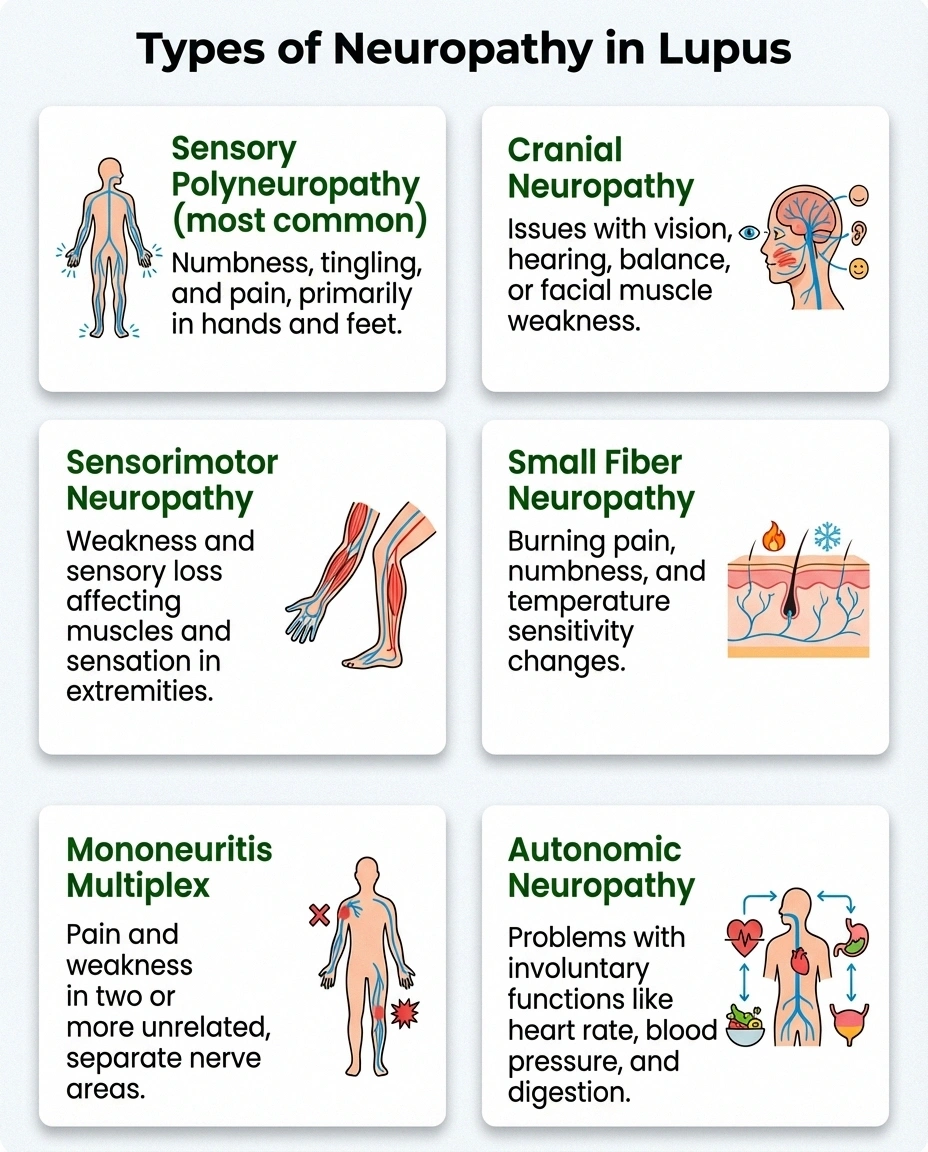
Sensory polyneuropathy is the most common form. It affects the longest nerves first — meaning symptoms typically start in your feet and hands, then gradually move upward. The classic “stocking-glove” distribution of numbness, tingling, and burning pain is the hallmark presentation. This pattern resembles diabetic neuropathy and other length-dependent neuropathies.
Sensorimotor neuropathy involves both sensory and motor nerves. In addition to numbness and pain, you may experience muscle weakness, difficulty walking, or trouble with fine motor tasks like buttoning a shirt. This form tends to be more functionally disabling.
Mononeuritis multiplex affects individual nerves in different, seemingly random locations. You might develop sudden weakness in one foot, then numbness in a hand, then pain along a specific nerve in your thigh. This “patchy” pattern is strongly associated with vasculitis and can be a red flag that lupus is actively inflaming blood vessels.
Cranial neuropathy affects the nerves emerging directly from the brain. In lupus, this can cause sudden facial weakness (similar to Bell's palsy), vision changes, hearing loss, or difficulty swallowing. Cranial neuropathies tend to respond more rapidly to treatment than peripheral neuropathies, according to the inception cohort study mentioned above.
Small fiber neuropathy affects the smallest nerve fibers responsible for pain, temperature sensation, and autonomic functions. This form may cause burning pain that's disproportionate to what standard nerve tests show — because standard EMG and nerve conduction studies can't detect small fiber damage. It requires a skin biopsy for definitive diagnosis.
Autonomic neuropathy affects the nerves controlling involuntary body functions. Symptoms include blood pressure fluctuations, rapid heart rate, digestive problems, excessive sweating or inability to sweat, and bladder dysfunction. In lupus, autonomic neuropathy often coexists with sensory neuropathy.
Recognizing the Symptoms
Lupus neuropathy symptoms can develop gradually over weeks to months, or they can appear suddenly — particularly with mononeuritis multiplex. The Lupus Foundation of America identifies these key symptoms:

Don't Dismiss New Symptoms
It's easy to attribute every new symptom to “just the lupus” — but new tingling, numbness, or weakness deserves specific evaluation. Lupus neuropathy is treatable, and early intervention leads to better outcomes. Tell your rheumatologist about any new nerve symptoms, even if they seem minor.
- Numbness and tingling in hands, feet, arms, or legs — often starting in the toes and fingertips
- Burning or electric shock pain — often worse at night, similar to other forms of neuropathic pain
- Muscle weakness — difficulty gripping objects, foot drop, or trouble climbing stairs
- Loss of balance and coordination — from impaired proprioception
- Sensitivity to touch — even light contact may feel painful (allodynia)
- Facial pain or weakness — suggests cranial nerve involvement
- Carpal tunnel syndrome — compression of the median nerve at the wrist, which occurs more frequently in lupus patients
- Digestive symptoms, dizziness on standing, or irregular heartbeat — signs of autonomic involvement
Because these symptoms overlap with many other conditions — fibromyalgia, medication side effects, vitamin deficiencies — it's critical to get a proper evaluation rather than assuming all new symptoms are “just the lupus.”
Getting a Diagnosis
Diagnosing lupus-related neuropathy requires confirming both that neuropathy is present and that lupus is the cause — not always straightforward when you may also have other risk factors like diabetes or vitamin deficiencies.

Diagnostic Tip
If you have burning pain with normal nerve conduction studies, ask about a skin biopsy. Small fiber neuropathy — which is common in lupus — can only be detected through a skin punch biopsy that counts the tiny nerve fibers in your skin. Standard EMG tests miss it entirely.
Nerve conduction studies and electromyography (EMG). These are the standard first-line tests. Nerve conduction studies measure how fast and how strongly electrical signals travel through your nerves, while EMG examines the electrical activity in your muscles. Together, they can identify which nerves are damaged, what type of damage is present, and how severe it is.
Blood work. Your doctor will typically check blood tests including inflammatory markers (ESR, CRP), complement levels (C3, C4), anti-dsDNA antibodies, and anti-neuronal antibodies. Low complement levels with elevated anti-dsDNA often indicate active lupus disease — which makes it more likely that the neuropathy is lupus-related rather than from another cause.
Skin biopsy. If small fiber neuropathy is suspected (burning pain with normal nerve conduction studies), a skin punch biopsy can count the small nerve fibers in your skin. Reduced fiber density confirms small fiber neuropathy.
Lumbar puncture. In some cases, a spinal tap may be performed to analyze your cerebrospinal fluid for signs of inflammation or immune system activity affecting the nervous system.
Ruling out other causes. Your doctor should also check for vitamin deficiencies (B12, folate, B6), blood sugar abnormalities, thyroid function, and medication side effects. Finding another cause doesn't rule out lupus neuropathy — but it changes the treatment approach.
Treatment Approaches
Treating lupus neuropathy involves two parallel strategies: controlling the underlying lupus disease activity that's causing nerve damage, and managing neuropathy symptoms directly.
Controlling Lupus Disease Activity
This is the foundation. If lupus-driven inflammation is actively damaging your nerves, no amount of symptom management will stop the progression. Treatment typically involves:
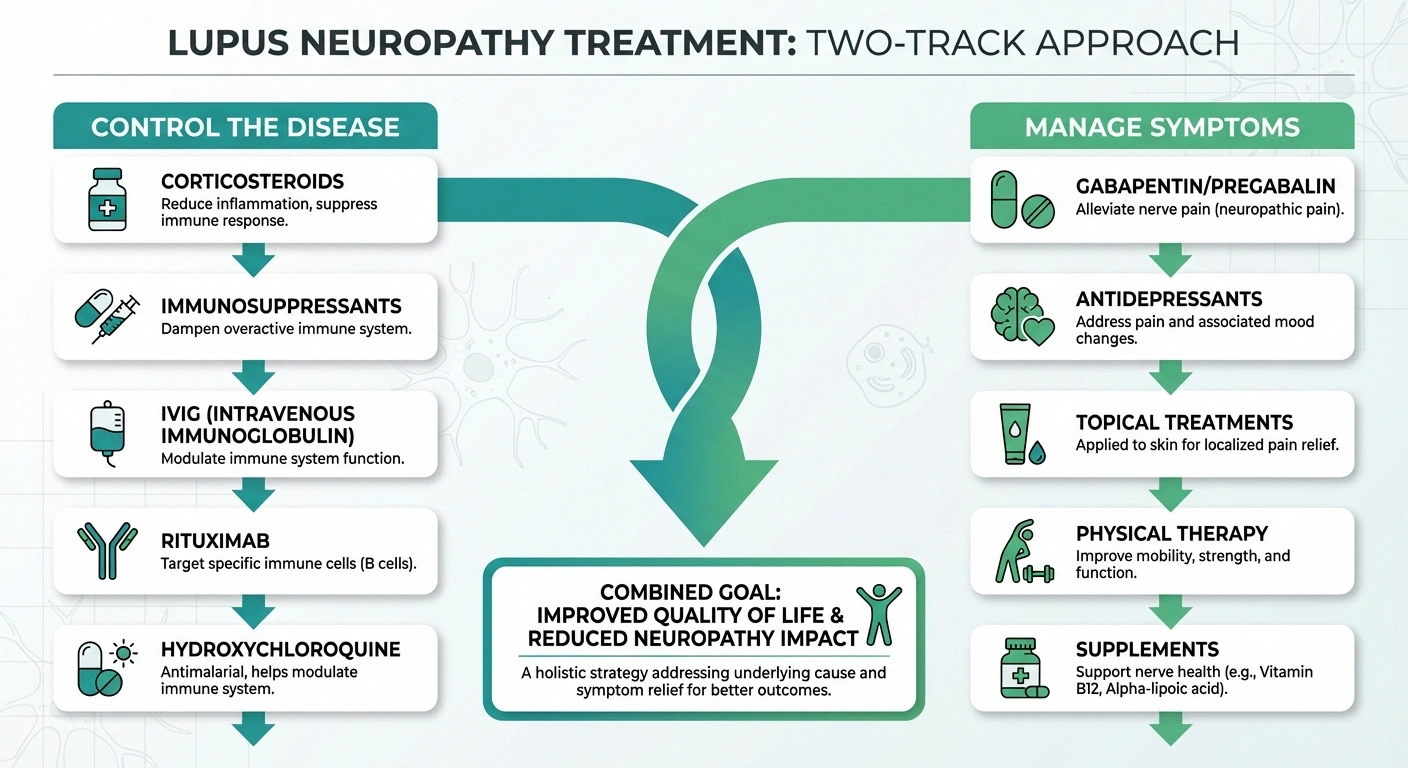
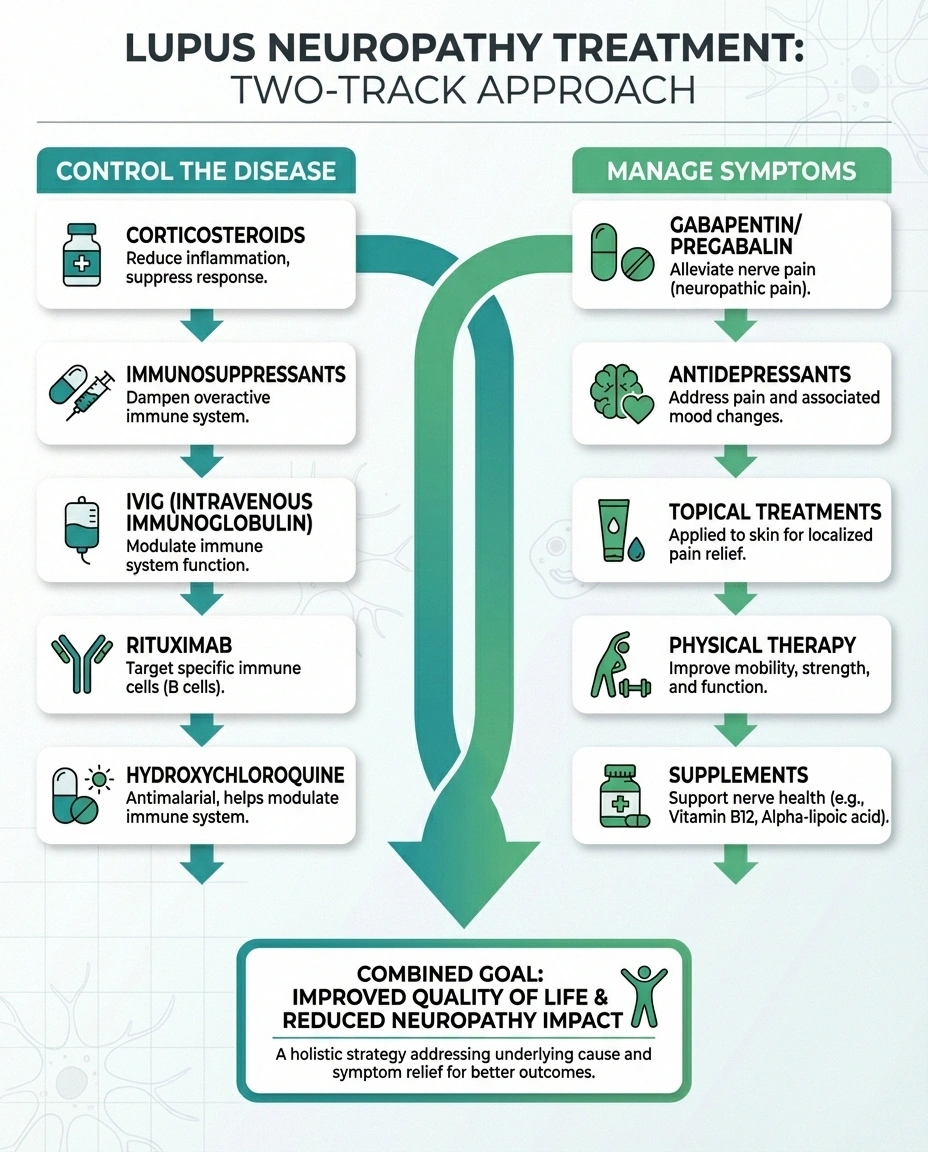
Two-Track Treatment
Lupus neuropathy treatment works on two parallel tracks: controlling the autoimmune disease (immunosuppressants) to stop ongoing nerve damage, and managing symptoms (gabapentin, duloxetine, topical treatments) for day-to-day relief. Both tracks are important — symptom management without disease control means the damage continues.
- Corticosteroids (prednisone, methylprednisolone) — often the first line for acute nerve damage, sometimes given intravenously for severe presentations. Effective at rapidly reducing inflammation, but long-term use carries significant side effects.
- Immunosuppressants — azathioprine, mycophenolate mofetil, or cyclophosphamide may be used to suppress the overactive immune response. The EULAR recommendations for neuropsychiatric lupus suggest glucocorticoids combined with immunosuppressive agents as the primary treatment approach.
- Intravenous immunoglobulin (IVIG) — infusions of concentrated antibodies from donated blood. Case reports and small studies have shown improvement in lupus neuropathy with IVIG, particularly for sensory neuronopathy. A case reported in the Journal of Medical Case Reports documented both clinical and electrophysiological improvement following IVIG treatment.
- Rituximab — a biologic medication that targets B cells (immune cells that produce antibodies). Used in refractory cases when other immunosuppressants haven't controlled the neuropathy.
- Hydroxychloroquine (Plaquenil) — the backbone of lupus treatment. While not specifically for neuropathy, maintaining overall disease control with hydroxychloroquine helps prevent new organ damage, including nerve damage.
Managing Neuropathy Symptoms
While immunosuppressive treatment targets the cause, you'll likely need additional medications and strategies to manage the pain and sensory symptoms. These are the same approaches used for other types of neuropathy:
- Gabapentin or pregabalin — first-line medications for neuropathic pain
- Duloxetine or amitriptyline — antidepressants that also reduce nerve pain
- Topical treatments — capsaicin cream or lidocaine patches for localized pain relief
- Physical therapy — to maintain strength, balance, and mobility
- Supportive supplements — alpha-lipoic acid, B vitamins, and other nerve-supportive nutrients (always discuss with your rheumatologist, as some supplements can interact with lupus medications)
Prognosis: What to Expect
The outlook for lupus neuropathy varies significantly depending on the type and severity. The good news: for many people, lupus neuropathy is at least partially reversible with proper treatment.
The international inception cohort study found that most lupus neuropathy cases showed improvement or resolution with treatment. Cranial neuropathies improved most rapidly. Sensory polyneuropathy and mononeuritis multiplex also showed significant improvement, though recovery was slower in patients with longer disease duration and older age at lupus diagnosis.
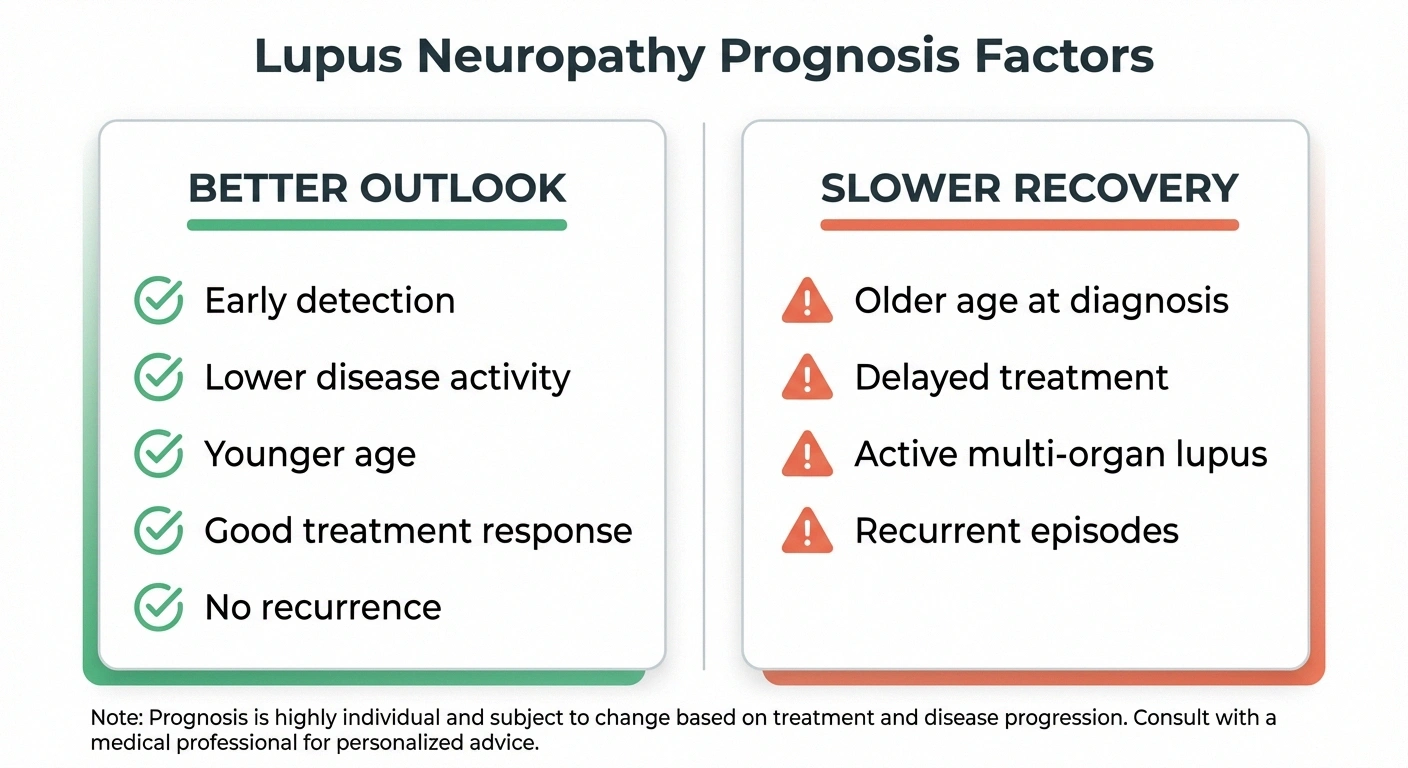
Factors associated with a better prognosis include:
- Early detection and prompt treatment
- Lower overall lupus disease activity
- Younger age at diagnosis
- Absence of recurrent neuropathy episodes
- Good response to initial immunosuppressive therapy
Factors associated with slower recovery:
- Older age at lupus diagnosis
- Longer delay between neuropathy onset and treatment
- Active lupus disease in other organs simultaneously
- Multiple or recurrent neuropathy episodes
Living with Lupus Neuropathy
Beyond medical treatment, there are practical strategies that can help you manage daily life with lupus-related nerve damage.

📋 Lupus Neuropathy Management Checklist
Protect your feet. Follow the same foot care guidelines recommended for any neuropathy — inspect your feet daily, wear well-fitting, supportive shoes, never go barefoot, and see a podiatrist at the first sign of any sore, blister, or skin change.
Stay active. Exercise is beneficial for both lupus and neuropathy, though you'll need to balance activity with lupus fatigue. Low-impact options like swimming, yoga, and walking can help maintain strength and circulation without overtaxing joints affected by lupus.
Monitor and communicate. Keep a symptom journal tracking your neuropathy symptoms alongside lupus flares. This helps your rheumatologist see whether neuropathy symptoms correlate with disease activity — critical information for adjusting treatment.
Address the emotional impact. Living with two chronic conditions simultaneously is emotionally taxing. Depression and anxiety are common in both lupus and neuropathy. Don't hesitate to seek support through counseling, support groups, or conversations with people who understand what you're going through.
Coordinate your care. Lupus neuropathy sits at the intersection of rheumatology and neurology. Make sure both specialists are communicating. Your rheumatologist manages the autoimmune disease; your neurologist monitors the nerve damage. Neither has the full picture alone.
Frequently Asked Questions
How common is neuropathy in lupus?
Studies report widely varying prevalence rates, from 3% to 28%, depending on the diagnostic methods used and the patient population studied. When sensitive diagnostic tools like nerve conduction studies and skin biopsies are used, higher rates of subclinical nerve damage are detected. A reasonable estimate is that approximately 5-15% of people with systemic lupus erythematosus will develop clinically significant peripheral neuropathy during their disease course.
Can lupus neuropathy be reversed?
In many cases, yes — at least partially. When lupus-driven inflammation is brought under control with immunosuppressive therapy, nerve damage may stabilize and, in some patients, partially reverse. The degree of recovery depends on how early treatment begins, the severity of damage, and how well lupus disease activity is controlled. Complete reversal is possible in mild cases caught early, while more established damage may improve but not fully resolve.
Is lupus neuropathy the same as diabetic neuropathy?
They share some symptoms — particularly the stocking-glove pattern of numbness and tingling in feet and hands — but the underlying mechanisms are completely different. Diabetic neuropathy is caused by metabolic damage from high blood sugar, while lupus neuropathy is caused by autoimmune inflammation and vasculitis attacking nerves. The distinction matters because the treatments differ fundamentally: lupus neuropathy requires immunosuppression, while diabetic neuropathy requires blood sugar control.
Should I see a neurologist if I have lupus and nerve symptoms?
Yes. While your rheumatologist manages lupus overall, a neurologist can perform the specialized testing needed to confirm neuropathy, identify the type and severity, rule out other causes, and monitor nerve function over time. Ask your rheumatologist for a referral to a neurologist experienced with autoimmune neuropathies. Early diagnosis and treatment lead to better outcomes.
Can lupus medications cause neuropathy?
Some lupus medications can contribute to nerve problems, including long-term high-dose corticosteroids and certain immunosuppressants. Hydroxychloroquine can very rarely cause neuromyopathy with long-term use. However, the benefit of controlling lupus disease activity — which prevents immune-mediated nerve damage — typically far outweighs the small risk of medication-related neuropathy. If you suspect a medication is causing new nerve symptoms, discuss this with your doctor rather than stopping treatment on your own.
When to Seek Urgent Care
Most lupus neuropathy develops gradually, but some presentations require urgent medical attention:

Seek Emergency Care Immediately If You Experience:
Do not wait for your next scheduled appointment. Call your rheumatologist's on-call line or go to the ER.
- Sudden severe weakness in a limb — may indicate mononeuritis multiplex or active vasculitis
- Sudden facial drooping or vision changes — cranial neuropathy needs immediate evaluation to rule out stroke
- Rapidly spreading numbness or weakness — ascending weakness could indicate Guillain-Barré syndrome, which can rarely occur alongside lupus
- Loss of bladder or bowel control — may indicate myelitis (spinal cord inflammation), a medical emergency
Don't wait for your next scheduled rheumatology appointment if you experience any of these symptoms. Go to the emergency room or call your rheumatologist's on-call line immediately. For a broader overview of neuropathy warning signs that need emergency attention, see our dedicated guide.
Living with lupus neuropathy means navigating two chronic conditions simultaneously — but it doesn't mean navigating them without a map. Work closely with your healthcare team, stay informed about your condition, and take an active role in managing both your autoimmune disease and your nerve health. Many people with lupus neuropathy see meaningful improvement with the right treatment approach, and the science of autoimmune neuropathy treatment continues to advance.