Peripheral Neuropathy: Symptoms, Causes, and Treatment Overview
If you've recently been diagnosed with peripheral neuropathy — or suspect you might have it — the sheer volume of information can feel overwhelming. Medical websites throw around terms like “axonal degeneration” and “demyelination” while offering frustratingly vague treatment advice. You deserve better than that.
I created this guide to be the comprehensive overview I wish existed when I first started learning about neuropathy. It covers what peripheral neuropathy actually is, the full range of symptoms you might experience, the most common causes, how it gets diagnosed, and every major treatment option — from prescription medications to evidence-based natural approaches. Consider this your home base for understanding this condition. Browse our complete guide to neuropathy types for deeper detail on specific forms.
What Is Peripheral Neuropathy?
Peripheral neuropathy is an umbrella term for any condition that damages the peripheral nerves — the vast network of nerves outside your brain and spinal cord. These nerves are your body's communication highways, carrying signals between your brain, spinal cord, and every other part of your body.
The National Institute of Neurological Disorders and Stroke (NINDS) identifies more than 100 types of peripheral neuropathy, each with distinct characteristics. But they all share one thing in common: something has damaged or disrupted the peripheral nerves' ability to send and receive signals properly.
That disruption can manifest in three ways: signals that should be sent aren't (numbness), signals sent when they shouldn't be (random pain or tingling), and errors that distort the messages (burning sensations, feeling like you're wearing a sock when you aren't). According to NINDS, peripheral neuropathy affects approximately 20 million people in the United States — though the actual number may be significantly higher because many cases go undiagnosed.
The Three Types of Peripheral Nerves
Understanding which type of nerve is affected helps explain why symptoms vary so dramatically from person to person. Your peripheral nervous system contains three categories of nerves, and neuropathy can affect any combination of them.
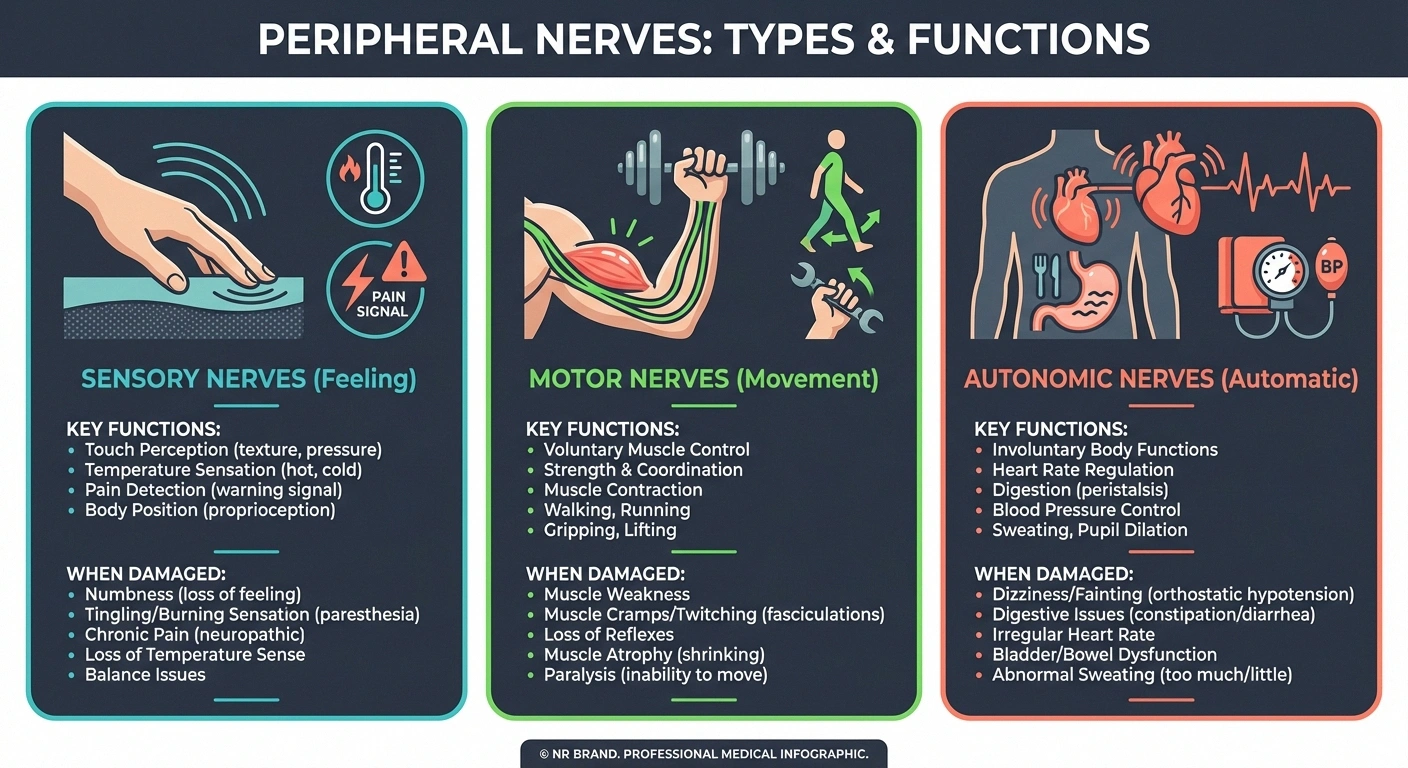
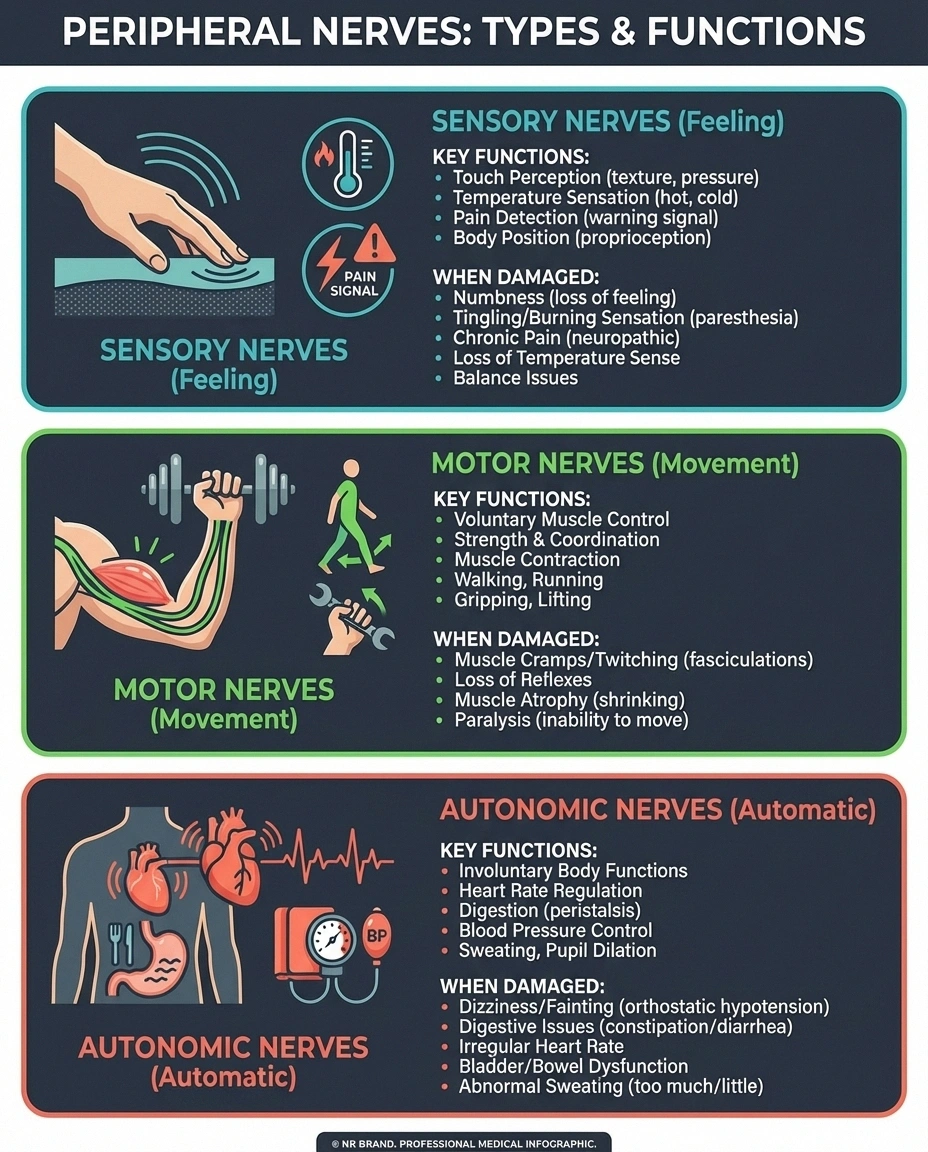
Sensory nerves transmit information about sensation — touch, temperature, pain, vibration, and your sense of body position (proprioception). When these are damaged, you experience numbness, tingling, burning, or pain. This is the type most people think of when they hear “neuropathy.”
Motor nerves control your voluntary muscles — the ones you consciously use for walking, gripping, talking, and every other deliberate movement. Damage to motor nerves causes weakness, cramps, muscle wasting, and difficulty with coordination. If you're having trouble with balance or noticing your muscles shrinking, motor nerves may be involved.
Autonomic nerves control everything you don't think about — heart rate, blood pressure, digestion, bladder function, sweating, and sexual response. Autonomic neuropathy can affect any of these systems, sometimes creating symptoms that seem completely unrelated to nerve damage.
Most neuropathies affect all three types to varying degrees, which is why a single person might experience tingling feet, muscle weakness, and digestive problems simultaneously.
Common Symptoms of Peripheral Neuropathy
Symptoms depend on which nerves are damaged and how severely. Most people experience a combination of sensory, motor, and sometimes autonomic symptoms. Here's a comprehensive breakdown of what neuropathy actually feels like for most people.
Sensory Symptoms
Numbness and tingling, usually starting in the toes or fingers, are the most commonly reported first symptoms. Many people describe a “pins and needles” sensation that doesn't go away. Burning pain — often worse at night — is another hallmark. Some people experience intensified symptoms at night that severely disrupt sleep. Other sensory symptoms include heightened sensitivity to touch (even a bedsheet can feel painful), electric shock sensations, a feeling of wearing invisible socks or gloves, and loss of ability to feel temperature changes — which creates a serious risk for burns and injuries.
Motor Symptoms
Muscle weakness, particularly in the feet and hands, develops as motor nerves are affected. Foot drop — difficulty lifting the front part of your foot — is a common sign. Muscle cramps, loss of coordination, and difficulty with fine motor tasks (buttoning a shirt, turning a key) are frequently reported. In advanced cases, visible muscle wasting occurs in the feet and legs.

Autonomic Symptoms
These are the symptoms many people don't realize are connected to neuropathy: dizziness when standing up (orthostatic hypotension), digestive issues like bloating, constipation, or diarrhea, bladder dysfunction, excessive sweating or inability to sweat, and sexual dysfunction. If you're experiencing these alongside sensory symptoms, mention them to your doctor — they provide important diagnostic information.
What Causes Peripheral Neuropathy?
There are dozens of known causes, which is part of what makes diagnosis challenging. In some cases — called idiopathic neuropathy — no cause can be identified despite thorough testing.
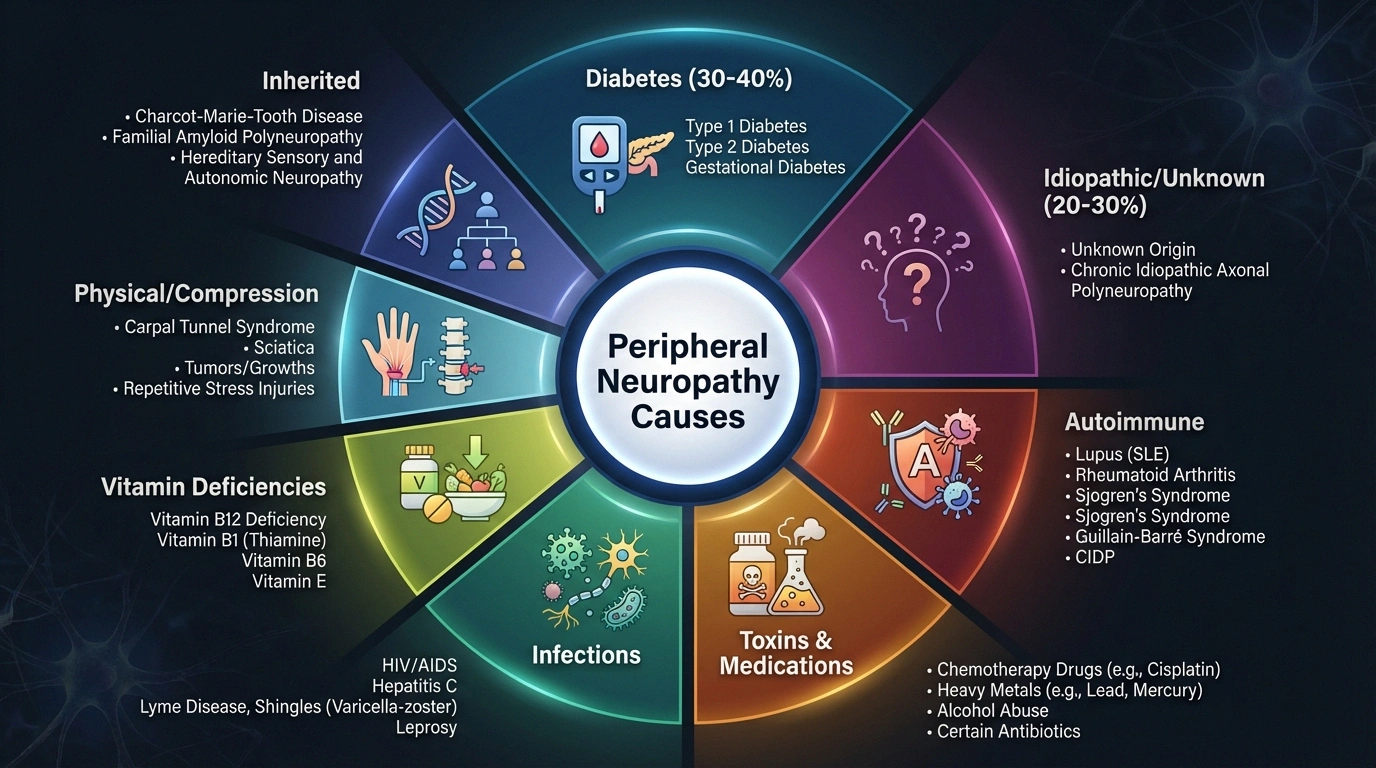
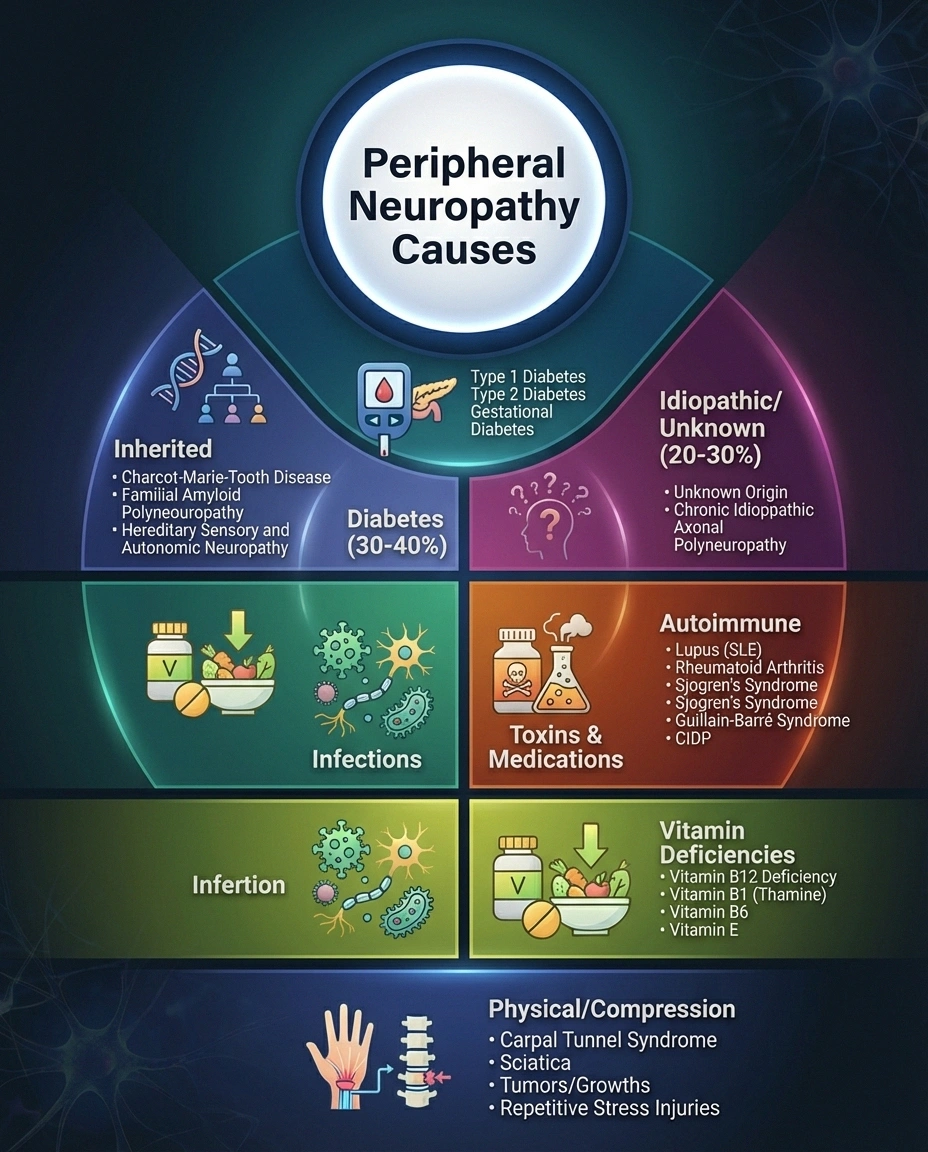
Diabetes
Diabetes is the single most common cause, responsible for approximately 30-40% of all peripheral neuropathy cases. High blood sugar damages the small blood vessels that supply nerves with oxygen and nutrients. Our complete guide to diabetic neuropathy covers this in detail. People with prediabetes can also develop neuropathy — nerve damage sometimes precedes a diabetes diagnosis.
Vitamin Deficiencies
B vitamins — especially B12, B1 (thiamine), and B6 — are essential for nerve health. Vitamin deficiency neuropathy is more common than many people realize, particularly in older adults, vegans, and people taking medications like metformin that deplete B12. Vitamin E and copper deficiency can also cause nerve damage.
Autoimmune Conditions
Conditions like Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy (CIDP), lupus, rheumatoid arthritis, and celiac disease can cause the immune system to attack nerve tissue. Autoimmune neuropathies can be acute (developing rapidly) or chronic (developing gradually over years).
Toxins and Medications
Chemotherapy is one of the most common medication-related causes — chemo-induced neuropathy (CIPN) affects 30-70% of cancer patients receiving certain drugs. Other medications that can cause neuropathy include certain antibiotics, statins, and anticonvulsants. Alcohol and industrial chemicals are also significant toxic causes.
Infections
Shingles (post-herpetic neuralgia), Lyme disease, HIV, hepatitis C, and COVID-19 can all damage peripheral nerves directly or through immune responses. Post-infectious neuropathies sometimes resolve as the body fights off the infection, but they can also persist long-term.
Physical Causes
Injuries, repetitive stress, and compression can damage individual nerves. Carpal tunnel syndrome is a common example of compression neuropathy. Surgery can inadvertently damage nearby nerves. Proximal neuropathy in the hips and thighs is another physical pattern, particularly in diabetes.
Inherited Conditions
Charcot-Marie-Tooth disease is the most common inherited neuropathy, affecting approximately 1 in 2,500 people. These genetic neuropathies typically develop gradually in childhood or early adulthood.
How Peripheral Neuropathy Is Diagnosed
Getting an accurate diagnosis usually involves multiple steps because there's no single test that confirms neuropathy. Here's what to expect.

Neurological examination: Your doctor will test reflexes, muscle strength, ability to feel various sensations (light touch, vibration, temperature, pinprick), and coordination. This clinical exam is the foundation of diagnosis.
Blood work: Lab tests for neuropathy typically include fasting glucose and HbA1c (for diabetes), vitamin B12 and folate levels, thyroid function, inflammatory markers, and sometimes tests for autoimmune conditions. A complete metabolic panel and CBC help rule out kidney disease, liver dysfunction, and other systemic causes.
Nerve conduction studies and EMG: Electromyography (EMG) and nerve conduction studies measure how quickly and efficiently your nerves transmit electrical signals. These tests can confirm neuropathy, determine whether it's axonal or demyelinating, and estimate severity.
Skin biopsy: A small punch biopsy that counts nerve fiber density in the skin. This is the gold standard for diagnosing small fiber neuropathy, which normal nerve conduction studies can miss.
Additional testing: Depending on your situation, your doctor might order imaging (MRI), lumbar puncture, or genetic testing. The goal is always to identify the underlying cause because treating the cause — when possible — is the most effective way to stop progression.
Prescription Medication Treatment Options
There is no single “neuropathy medication” — treatment targets either the underlying cause or the symptoms (primarily pain). Our complete guide to neuropathy medications covers every option in detail, but here's the essential overview.
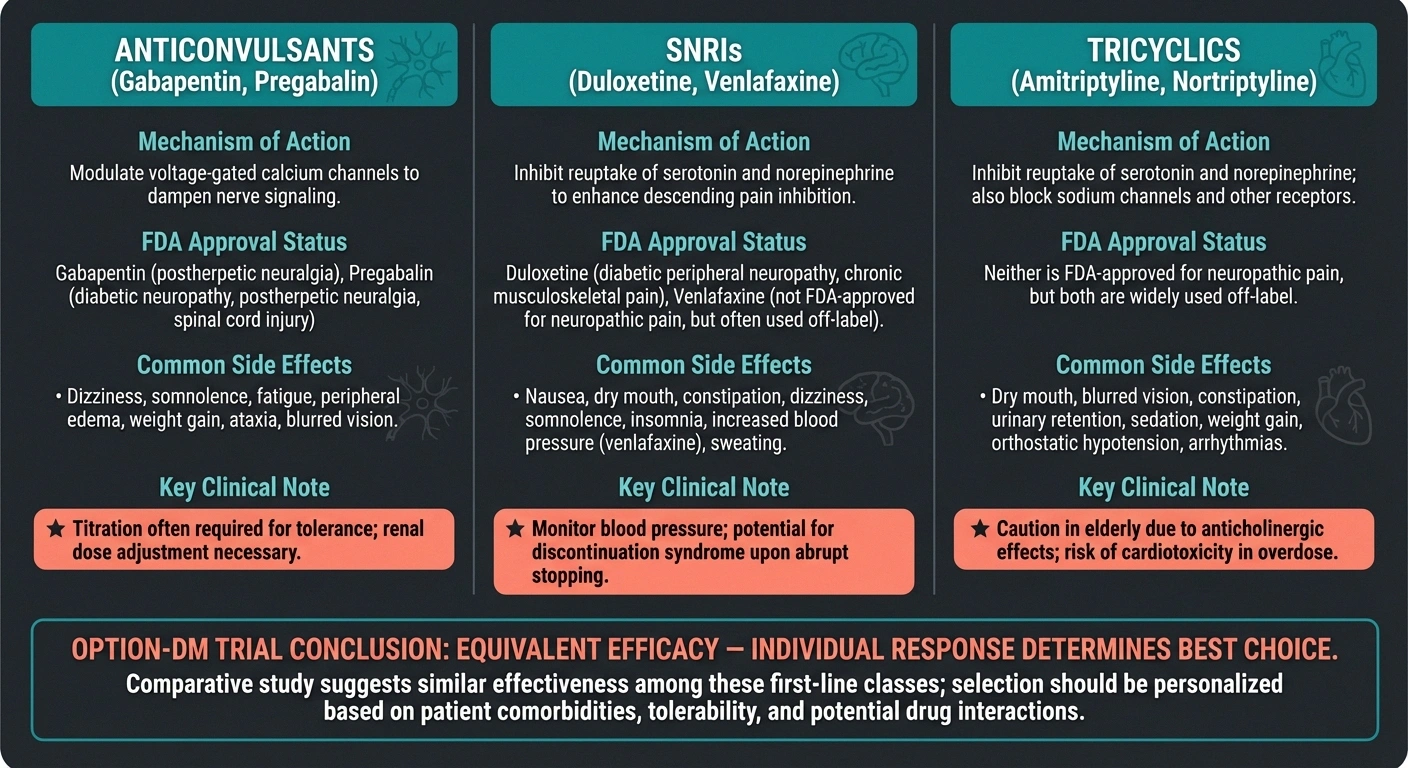

First-Line Pain Medications
The three drug classes most commonly prescribed as first-line treatments are anticonvulsants (gabapentin, pregabalin), SNRIs (duloxetine, venlafaxine), and tricyclic antidepressants (amitriptyline, nortriptyline). The FDA has specifically approved pregabalin and duloxetine for diabetic neuropathic pain, though all of these medications are widely used for neuropathy of any cause.
The OPTION-DM trial, one of the largest comparative studies of neuropathy pain medications, found that these drug classes have equivalent overall efficacy — meaning no single medication is clearly superior. What works best varies from person to person. If the first medication doesn't help or causes intolerable side effects, your doctor will try another. Combination therapy (using two drug classes together) provided significantly better pain relief for patients who didn't respond adequately to a single medication.
Topical Treatments
Lidocaine patches and capsaicin cream provide localized pain relief without systemic side effects. High-concentration capsaicin (8%) patches, applied by a healthcare provider, have shown meaningful pain reduction lasting up to 3 months per application. These are particularly useful for people who can't tolerate oral medications.
Advanced Interventions
For severe, treatment-resistant pain, spinal cord stimulation and scrambler therapy offer options when medications haven't provided adequate relief. Spinal cord stimulation has been FDA-approved for painful diabetic neuropathy, with studies showing significant pain reduction and improved quality of life.
Natural and Complementary Treatments
Evidence-based natural treatments can complement — and sometimes replace — prescription medications. Our complete guide to natural remedies for neuropathy covers the full range, but here are the approaches with the strongest evidence.

Alpha-lipoic acid (ALA) is the most-studied natural supplement for neuropathy. Multiple randomized controlled trials have demonstrated that 600mg daily of alpha-lipoic acid reduces neuropathic pain, burning, and numbness — particularly in diabetic neuropathy. It works as a powerful antioxidant that protects nerve cells from oxidative damage.
B vitamin supplementation is essential when deficiency is a factor. Our B vitamin guide covers dosing for B1, B6, and B12 specifically for nerve health. B12 injections may be necessary when oral absorption is impaired.
Exercise has growing evidence as a neuropathy intervention. Walking, swimming, yoga, and physical therapy all show benefits for pain reduction, improved balance, and nerve function — potentially even nerve regeneration. Exercise may be the single most underutilized treatment for neuropathy.
Other evidence-based approaches include acupuncture (moderate evidence for pain relief), TENS units (electrical nerve stimulation), infrared therapy, and magnesium supplementation.
Living with Peripheral Neuropathy
Managing neuropathy is a daily practice, not a one-time fix. For a more complete look at daily strategies, see our guide to living well with neuropathy. Here are the fundamentals.

Foot care is non-negotiable. When you can't feel your feet properly, injuries go unnoticed. Daily foot inspections, proper footwear, and never walking barefoot are essential to preventing complications. Our neuropathy foot care guide covers everything you need to know.
Fall prevention matters. With impaired sensation and balance, fall prevention becomes a critical safety concern. Simple home modifications — grab bars, good lighting, removing rugs — can prevent serious injuries.
Sleep management. Since neuropathy and sleep problems often go hand-in-hand, developing good sleep hygiene and working with your doctor to manage nighttime pain is important for overall quality of life.
Mental health support. Chronic pain takes a toll on mental health. Depression, anxiety, and grief about lost abilities are normal responses. Cognitive behavioral therapy and mindfulness practices have evidence for improving both pain and emotional well-being in neuropathy patients.
What to Expect: Prognosis and Progression
The natural question after diagnosis is: “What's going to happen to me?” The honest answer is that neuropathy prognosis varies enormously depending on the cause.
Reversible causes: Neuropathy from vitamin deficiency, medication side effects, or compression can often be partially or fully reversed by addressing the cause. Nerve regeneration is possible — peripheral nerves can regrow at about 1mm per day — but recovery is slow and may take months to years.
Manageable causes: Diabetic neuropathy and autoimmune neuropathies can often be stabilized and managed, even if complete reversal isn't possible. Tight blood sugar control in diabetes, for example, can prevent further progression and may even allow some recovery. Learn more about neuropathy reversibility.
Progressive conditions: Inherited neuropathies and some idiopathic forms may progress gradually over time. Even in these cases, treatment can manage symptoms and slow progression. No neuropathy diagnosis is a reason to give up on improvement.
Regardless of cause, early intervention consistently leads to better outcomes. If you suspect neuropathy, don't wait — see a doctor. If your primary care physician isn't taking your symptoms seriously, know that seeing a neurologist may be your best next step.
Frequently Asked Questions
Is peripheral neuropathy a disability?
Peripheral neuropathy can be disabling depending on severity, but having the diagnosis alone doesn't automatically qualify you for disability benefits. Severe cases affecting mobility, hand function, or causing debilitating pain may qualify for SSDI or SSI. The key is documenting how neuropathy specifically limits your ability to work through medical records, nerve conduction studies, and functional assessments.
Does peripheral neuropathy get worse over time?
Not necessarily. Whether neuropathy progresses depends entirely on the cause and whether it can be addressed. If the cause is ongoing (uncontrolled diabetes, continued alcohol use, ongoing toxic exposure), yes, it typically worsens. If the cause is removed or treated, many people stabilize and some improve. Even idiopathic neuropathy doesn't inevitably worsen — some cases remain stable for years.
Can peripheral neuropathy be cured?
Some forms can be fully reversed: neuropathy from vitamin B12 deficiency (when caught early and treated), compression neuropathies (when the pressure is relieved), and some medication-induced cases (when the medication is stopped). Most forms are treatable but not curable in the traditional sense. The focus shifts to managing symptoms, preventing progression, and maximizing quality of life.
What is the best treatment for peripheral neuropathy?
There is no single best treatment — the optimal approach depends on your specific cause and symptoms. The most effective strategy is almost always a combination: treat the underlying cause (if known), manage pain with appropriate medication, supplement any nutritional deficiencies, maintain physical activity, and address lifestyle factors. What works for one person may not work for another, and finding the right combination often requires patience.
Should I see a neurologist or can my primary care doctor treat neuropathy?
Primary care doctors can manage straightforward cases — especially when the cause is clear (like diabetes) and symptoms are mild. A neurologist referral is warranted when the cause is unknown, symptoms are severe or progressing rapidly, standard treatments aren't helping, or you need nerve conduction studies or skin biopsy for diagnosis. A neurologist has specialized training in nerve diseases and access to diagnostic tools your primary care doctor may not have.
How common is peripheral neuropathy?
It's far more common than most people realize. NINDS estimates approximately 20 million Americans have peripheral neuropathy, but the actual number is likely higher because mild cases often go undiagnosed. The prevalence increases significantly with age — studies suggest up to 8% of people over 55 have some form of peripheral neuropathy. Among people with diabetes, the rate is dramatically higher: 30-50% depending on duration and blood sugar control.